
Periodontal pockets are a common dental condition associated with periodontal disease, also known as gum disease. These pockets are spaces or gaps that develop between the teeth and the surrounding gum tissue due to the destruction of the supporting periodontal structures. They are not only a sign of gum disease but also serve as a breeding ground for bacteria, further exacerbating the condition. If left untreated, periodontal pockets can lead to severe consequences including tooth loss and systemic health issues.
Table of Contents
ToggleWhat Is a Periodontal Pocket?
A periodontal pocket is a pathological deepening of the natural space that exists between a tooth and the surrounding gum tissue. This space, called the gingival sulcus, is present even in a healthy mouth. Under normal conditions, the sulcus is shallow measuring approximately 1 to 3 millimeters in depth and is lined with healthy epithelium that acts as a barrier against bacteria and other external irritants.
When a person develops periodontal disease—particularly periodontitis, the more advanced form of gum disease—this sulcus can become abnormally deep. The increased depth occurs due to the breakdown of the connective tissue and bone that anchor the tooth to the jawbone. This degradation leads to a larger gap between the gum and the tooth, forming what is referred to as a periodontal pocket.
These pockets are not merely deeper grooves; they represent sites of active infection and inflammation. Inside these pockets, harmful bacteria thrive, leading to further destruction of the tissues that support the tooth. The condition becomes self-perpetuating: as the pocket deepens, it becomes more difficult to clean effectively, which leads to more plaque accumulation, more bacteria, more inflammation, and even deeper pockets.
Gingival Sulcus vs. Periodontal Pocket
| Feature | Healthy Gingival Sulcus | Periodontal Pocket |
|---|---|---|
| Depth | 1–3 mm | 4 mm or more |
| Tissue Health | Intact, tight junction | Inflamed, detached from tooth |
| Bacterial Activity | Low or controlled | High, with pathogenic species |
| Plaque Accumulation | Easily removed by brushing/flossing | Difficult to remove, often retained |
| Bone Involvement | None | Often accompanied by bone loss |
How a Periodontal Pocket Forms: Step-by-Step Breakdown
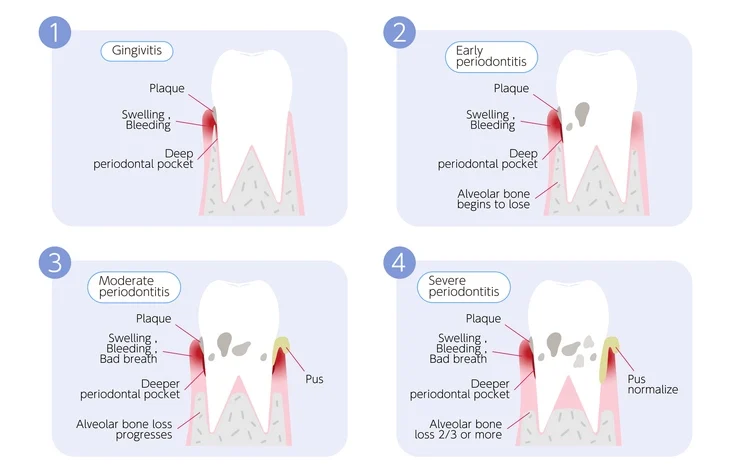
- Plaque Accumulation: Poor oral hygiene allows plaque (a biofilm of bacteria) to accumulate along the gumline.
- Gingival Inflammation: The bacteria in plaque release toxins that irritate the gum tissue, causing gingivitis—red, swollen, and bleeding gums.
- Attachment Loss: Continued inflammation triggers the body’s immune response. The immune system releases enzymes and inflammatory mediators that begin to destroy the connective tissue and bone.
- Formation of the Pocket: As the gum tissue detaches from the tooth and bone is resorbed, the depth of the sulcus increases, creating a periodontal pocket.
- Bacterial Colonization: The pocket becomes a favorable environment for anaerobic, pathogenic bacteria that thrive in oxygen-poor, protected environments.
- Progression: Without intervention, the pocket deepens further, leading to advanced periodontal disease, tooth mobility, and potentially tooth loss.
Types of Periodontal Pockets
Periodontal pockets can be classified based on their location relative to the alveolar bone and other anatomical features.
1. Suprabony (Supracrestal) Pocket
- Location: The bottom of the pocket is above the level of the alveolar bone.
- Pattern of Bone Loss: Horizontal.
- Common in: Early to moderate periodontitis.
2. Infrabony (Subcrestal or Intrabony) Pocket
- Location: The bottom of the pocket is below the level of the alveolar bone.
- Pattern of Bone Loss: Vertical.
- More Complex: These pockets often require surgical intervention or regenerative procedures.
3. Gingival Pocket (Pseudo-pocket)
- Not True Periodontal Pocket: Occurs when there is inflammation and swelling of the gingiva without actual attachment loss.
- Seen in: Gingivitis.
- Reversible: With proper care, these pockets can be resolved without long-term damage.
Clinical Implications of Periodontal Pockets
A periodontal pocket is not just a diagnostic marker—it is a functional risk factor. Its presence signifies ongoing tissue destruction and poses several serious clinical implications:
- Reservoir for Pathogens: The environment of the pocket allows anaerobic and gram-negative bacteria to flourish, making infection control more difficult.
- Chronic Inflammation: The body’s immune system is in a constant state of activity, which can spill over into systemic inflammation.
- Risk of Tooth Loss: Progressive loss of supporting structures leads to loose teeth, eventually necessitating extraction.
- Association with Systemic Disease: Deep periodontal pockets are associated with increased systemic inflammatory burden, and have been linked with conditions like diabetes, cardiovascular disease, and adverse pregnancy outcomes.
- Complicates Dental Treatments: Periodontal pockets can make it harder to fit crowns, bridges, or orthodontic appliances and may compromise implant success.
Pocket Depth and Disease Severity
Probing pocket depth (PPD) is a critical measurement in diagnosing periodontal disease and planning treatment. It is performed using a periodontal probe, a slender instrument marked in millimeters.
| Pocket Depth (mm) | Clinical Interpretation |
|---|---|
| 1–3 mm | Normal sulcus (healthy) |
| 4 mm | Early sign of periodontal involvement |
| 5–6 mm | Moderate periodontitis |
| 7 mm or more | Severe periodontitis, often with bone loss |
Pocket depth is often assessed alongside other parameters such as clinical attachment level (CAL), bleeding on probing (BOP), mobility, and furcation involvement to create a comprehensive periodontal chart.
Why Periodontal Pockets Are Difficult to Manage
Managing periodontal pockets poses unique challenges:
- Limited Access: Deeper pockets are hard to clean with regular brushing and flossing.
- Biofilm Resistance: Mature plaque biofilms are more resistant to mechanical removal and antimicrobials.
- Chronic Nature: Periodontal pockets often require long-term maintenance and monitoring.
- Tissue Changes: Pockets may involve both soft and hard tissue destruction, requiring complex interventions including surgery or grafting.
Microscopic View of a Periodontal Pocket
Under the microscope, a periodontal pocket is a zone of active destruction. Common histological features include:
- Ulcerated epithelium: The inner lining of the pocket is often ulcerated and allows bacterial toxins to enter the connective tissue.
- Inflammatory infiltrate: Neutrophils, lymphocytes, and plasma cells are commonly found, reflecting an active immune response.
- Bacterial invasion: Advanced cases show bacterial penetration into the soft tissue, making eradication more difficult.
Causes of Periodontal Pockets
The development of periodontal pockets is a result of the complex interplay between microbial biofilm (dental plaque), the host’s immune response, and a variety of environmental and systemic factors. Understanding these causes in detail not only aids in early detection and prevention but also informs the selection of appropriate treatment strategies.
1. Dental Plaque and Biofilm Formation
At the core of periodontal pocket formation is dental plaque, a biofilm of bacteria and extracellular matrix that adheres to the tooth surface. This biofilm is not just a passive accumulation but a dynamic microbial community that undergoes maturation over time:
- Early plaque is predominantly composed of gram-positive cocci and rods.
- Mature plaque includes gram-negative anaerobes such as Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola, which are strongly associated with periodontitis.
These bacteria release toxins and enzymes, such as lipopolysaccharides (LPS), collagenases, and proteases, that damage epithelial cells and connective tissue. The chronic inflammatory response to these bacterial products leads to destruction of the periodontal ligament and alveolar bone, creating a pocket.
2. Calculus (Tartar) Accumulation
When plaque is not regularly removed, it calcifies to form dental calculus. Calculus has a rough surface that promotes further plaque retention and harbors bacteria. Subgingival calculus, in particular, is directly associated with pocket formation as it is in close contact with the soft tissue wall and promotes chronic inflammation.
3. Host Immune Response and Inflammation
While the bacteria initiate the disease, the host’s immune response is responsible for much of the tissue destruction. The body attempts to fight the bacterial invasion using neutrophils, macrophages, and lymphocytes. However, in chronic cases:
- Excessive production of inflammatory cytokines like interleukin-1 (IL-1), tumor necrosis factor-alpha (TNF-α), and prostaglandin E2 (PGE2) leads to the breakdown of collagen and bone.
- Matrix metalloproteinases (MMPs) are enzymes that degrade extracellular matrix components, contributing to connective tissue loss.
Thus, an overactive or dysregulated immune response can paradoxically accelerate tissue destruction and deepen periodontal pockets.
4. Poor Oral Hygiene Practices
Inadequate brushing and flossing allow plaque to accumulate, particularly in hard-to-reach areas like molars or between teeth. Individuals who neglect daily oral care are at significantly higher risk of gingivitis progressing to periodontitis. Even those who brush regularly may fail to effectively clean along the gumline or between teeth, where plaque tends to accumulate.
5. Smoking and Tobacco Use
Tobacco is one of the most potent risk factors for periodontal disease. It contributes to pocket formation in several ways:
- Impairs neutrophil function, reducing the body’s ability to fight infection.
- Decreases blood flow to the gums, impairing nutrient delivery and healing.
- Alters the composition of the oral microbiome, favoring more pathogenic species.
Smokers often exhibit deeper pockets, greater bone loss, and more tooth loss compared to non-smokers, even when controlling for plaque levels.
6. Systemic Diseases
Several systemic conditions can exacerbate or predispose individuals to periodontal disease and pocket formation:
- Diabetes Mellitus: Poorly controlled diabetes increases susceptibility to infections and impairs wound healing, leading to more severe periodontal destruction. Hyperglycemia affects collagen metabolism and enhances inflammatory cytokine production.
- HIV/AIDS: Immune suppression in HIV-positive individuals results in more aggressive forms of periodontal disease, such as necrotizing ulcerative periodontitis.
- Osteoporosis: Reduced bone mineral density may increase alveolar bone loss, although the link is still being explored.
- Cardiovascular disease: There’s a bidirectional relationship between periodontal disease and heart health, possibly due to shared inflammatory pathways.
7. Hormonal Changes
Hormonal fluctuations can increase gum sensitivity and the response to bacterial plaque. While not a direct cause of periodontal pockets, hormonal changes can exacerbate existing inflammation:
- Puberty: Increased levels of sex hormones can lead to exaggerated gingival responses.
- Pregnancy: Pregnancy gingivitis is common due to increased progesterone levels, which enhance vascular permeability and tissue response.
- Menopause: Reduced estrogen levels can lead to dry mouth and bone resorption, both of which may contribute to periodontal deterioration.
8. Genetic Predisposition
Genetics play a significant role in individual susceptibility to periodontal disease. Some people inherit a hyper-responsive immune system that overreacts to bacterial biofilms, leading to more rapid tissue breakdown.
- Specific gene polymorphisms in IL-1, TNF-α, and Fcγ receptors have been associated with increased risk of periodontitis.
- A positive family history of periodontal disease can be a predictive factor, particularly in aggressive forms of periodontitis.
9. Occlusal Trauma and Malocclusion
Abnormal biting forces or misaligned teeth can contribute to localized pocket formation by:
- Damaging the periodontal ligament and supporting structures.
- Creating areas that are difficult to clean, allowing plaque to accumulate.
Although occlusal trauma alone does not initiate periodontal pockets, it can exacerbate existing inflammation and accelerate tissue breakdown when periodontal disease is present.
10. Stress
Chronic stress has been associated with increased levels of cortisol, a hormone that suppresses immune function. Stress can lead to:
- Poor oral hygiene practices due to neglect or fatigue.
- Reduced immune response, increasing susceptibility to periodontal infections.
Psychological stress has also been correlated with higher plaque scores and deeper periodontal pockets in several studies.
11. Nutritional Deficiencies
A diet lacking in essential nutrients—especially vitamin C, vitamin D, calcium, and omega-3 fatty acids—can compromise immune function and tissue repair, increasing the risk of periodontal disease:
- Vitamin C deficiency can lead to scurvy, characterized by bleeding gums and collagen breakdown.
- Vitamin D and calcium are essential for maintaining bone health; deficiency may contribute to alveolar bone loss.
12. Medications
Certain medications can contribute to periodontal pocket formation by affecting the gums and oral environment:
- Phenytoin (for epilepsy), cyclosporine (for organ transplants), and calcium channel blockers (e.g., nifedipine) are known to cause gingival overgrowth, which creates pseudo-pockets where plaque can accumulate.
- Antidepressants, antihistamines, and diuretics can cause xerostomia (dry mouth), reducing the protective effect of saliva and promoting bacterial colonization.
13. Inadequate Dental Work and Restorations
Ill-fitting crowns, bridges, or overhanging restorations can create niches where plaque accumulates and remains undisturbed, fostering bacterial growth and inflammation. Over time, this can lead to localized periodontal pocket formation.
14. Aging
While age itself is not a direct cause of periodontal disease, the cumulative exposure to risk factors over time, combined with decreased immune function and possible comorbidities, can increase susceptibility to periodontal pocket development in older adults.
Summary of Contributing Factors
| Category | Examples |
|---|---|
| Microbial | Dental plaque, pathogenic bacteria |
| Host Response | Immune system overreaction, cytokines, MMPs |
| Local Factors | Poor oral hygiene, calculus, malocclusion, faulty restorations |
| Systemic Conditions | Diabetes, HIV/AIDS, cardiovascular disease |
| Lifestyle | Smoking, alcohol use, stress |
| Hormonal Changes | Puberty, pregnancy, menopause |
| Genetic Factors | Family history, specific gene polymorphisms |
| Medications | Phenytoin, calcium channel blockers, immunosuppressants, xerostomic drugs |
| Nutritional Deficiency | Low vitamin C, D, calcium, or omega-3 |
Symptoms of Periodontal Pockets
Recognizing the symptoms of periodontal pockets is critical for early diagnosis and intervention. Unfortunately, periodontal disease—and the pockets it causes—often progresses silently and painlessly in its early stages. Many people are unaware they have a problem until significant damage has already occurred. However, as periodontal pockets deepen and the disease advances, a range of clinical signs and symptoms become apparent.
These symptoms vary in intensity and presentation depending on the depth of the pockets, the extent of tissue destruction, and individual immune response. Below is a comprehensive look at the symptoms associated with periodontal pockets and what they indicate about the underlying condition.
1. Bleeding Gums
Bleeding gums are often one of the first noticeable signs of gingival inflammation and early periodontal disease. In healthy gums, bleeding during brushing, flossing, or eating hard foods is uncommon. However, when periodontal pockets are present:
- The pocket lining becomes ulcerated and fragile due to chronic inflammation.
- Even gentle probing or brushing may cause noticeable bleeding.
- Bleeding may also occur spontaneously in severe cases.
Persistent bleeding is not only a local sign of inflammation but also an indication that the immune system is actively fighting off a bacterial invasion in the pocket.
2. Red, Swollen, or Tender Gums
As periodontal disease progresses, the gums may become:
- Red or purplish: Healthy gums are pale pink. Redness indicates increased blood flow due to inflammation.
- Swollen or puffy: Inflammatory fluid accumulates in the gingival tissues.
- Tender or painful: In some cases, patients report discomfort or soreness when touching the gums, chewing, or brushing.
Swelling may be localized to specific teeth where pockets have formed or generalized throughout the mouth.
3. Persistent Bad Breath (Halitosis)
Chronic halitosis is a common and socially distressing symptom of periodontal pockets. It results from:
- The accumulation of anaerobic bacteria in deep pockets.
- Production of volatile sulfur compounds (VSCs) like hydrogen sulfide and methyl mercaptan.
- Necrotic tissue and pus within infected pockets.
Patients may also report a bad taste in the mouth, especially in the morning or after eating, due to bacterial waste and decaying tissue trapped in the pockets.
4. Gum Recession
Gum recession refers to the apical (downward) movement of the gum margin away from the crown of the tooth. In the presence of periodontal pockets:
- The supporting tissues are destroyed, causing the gums to shrink.
- More of the tooth surface—and sometimes the root—is exposed.
- This can lead to sensitivity to temperature changes, sweets, or touch.
- It also makes the teeth appear longer, which may be of cosmetic concern to some patients.
Recession not only indicates tissue loss but also often corresponds with deeper underlying pockets that may not be easily visible.
5. Tooth Sensitivity
As the roots of the teeth become exposed due to gum recession or pocket formation, patients often experience heightened sensitivity. This sensitivity can occur in response to:
- Cold air or water
- Hot beverages
- Sweet or acidic foods
- Toothbrushing or flossing
The root surface is covered by cementum, which is much softer and less protective than enamel, making it more susceptible to wear and stimuli when exposed.
6. Tooth Mobility or Loosening
One of the most alarming symptoms of advanced periodontal pockets is increased tooth mobility. This occurs due to:
- Progressive loss of attachment from the periodontal ligament.
- Destruction of the alveolar bone that supports the teeth.
- Widening of the periodontal ligament space due to inflammation.
Initially, patients may notice slight movement or a “loose feeling” when biting. As the disease progresses, teeth may visibly shift position or move during chewing and speaking. Severe cases may result in tooth migration, flaring, or eventual tooth loss.
7. Formation of Gaps Between Teeth
As the bone and tissue between teeth deteriorate, spaces may develop that were not previously present. This phenomenon, often referred to as pathologic tooth migration, includes:
- Gaps or diastemas appearing between front teeth.
- Teeth that seem to spread out or tilt.
- A change in the way the upper and lower teeth fit together (bite misalignment).
These changes can impact both function and aesthetics, potentially leading to difficulty chewing and self-consciousness about appearance.
8. Pus or Exudate Between Teeth and Gums
In more severe cases of periodontitis, pus may be seen oozing from the gums. This indicates the presence of a periodontal abscess, a localized collection of infection.
- Pus is typically yellowish or greenish and may have an unpleasant odor.
- Patients may feel pressure or pain in the area, though some abscesses are painless.
- The affected area may appear swollen or red, and draining pus may be visible along the gumline.
The presence of pus signifies an advanced stage of periodontal destruction and requires immediate dental attention.
9. Pain When Chewing or Biting
Pain or discomfort when biting down can result from several factors related to periodontal pockets:
- Inflammation of the periodontal ligament.
- Loosened teeth shifting under pressure.
- Presence of abscesses or infected tissue.
- Exposure of sensitive root surfaces.
This symptom can range from mild tenderness to sharp, shooting pain and often correlates with deep, inflamed pockets or active infection.
10. Change in the Fit of Dentures or Dental Appliances
For denture wearers or those with dental bridges or partials, changes in fit may occur as a result of shifting teeth and loss of bone support. Symptoms include:
- Dentures feeling loose or uncomfortable.
- Difficulty chewing or speaking.
- The need for more frequent adjustments or relining.
These changes may signal underlying periodontal deterioration and pocket formation beneath the appliance.
11. Aesthetic Changes and Cosmetic Concerns
Periodontal pockets can have visible effects on a person’s smile, including:
- “Black triangles” between teeth caused by loss of papilla (gum tissue between teeth).
- Tooth elongation due to recession.
- Discoloration or staining of exposed root surfaces.
- Shifting teeth that disrupt natural tooth alignment.
While these changes are not always painful, they can cause emotional and psychological distress for many patients.
12. Asymptomatic Progression (The “Silent Disease”)
Perhaps one of the most insidious aspects of periodontal pockets is their tendency to progress without noticeable symptoms, especially in the early stages. Many individuals may not be aware of any problems until:
- They visit a dentist for a routine check-up.
- They experience sudden pain, mobility, or abscess formation.
- They notice visible changes in tooth alignment or gum appearance.
This “silent” nature underscores the importance of regular dental examinations and periodontal probing to detect pockets before irreversible damage occurs.
When to Seek Professional Help
If you experience any of the following symptoms consistently, it is critical to consult with a dental professional:
- Bleeding while brushing or flossing
- Red, swollen, or receding gums
- Persistent bad breath or bad taste
- Loose or shifting teeth
- Pain when chewing
- Visible pus or discharge near the gums
Early intervention can significantly improve outcomes and may help prevent the need for more invasive procedures like surgery or tooth extraction.
Diagnosis of Periodontal Pockets
Diagnosing periodontal pockets is a critical step in identifying periodontal disease and formulating an effective treatment plan. Since periodontal pockets are often asymptomatic in their early stages, clinical examination by a dental professional is essential. The diagnosis is based on a combination of visual, tactile, radiographic, and sometimes microbiological assessments.
A thorough periodontal examination not only confirms the presence of pockets but also evaluates the extent and severity of tissue destruction, bone loss, and overall periodontal health.
1. Periodontal Probing
Periodontal probing is the cornerstone of diagnosing periodontal pockets. It involves the use of a periodontal probe, a thin, blunt, graduated instrument marked in millimeters.
a. Technique
- The probe is gently inserted into the gingival sulcus between the tooth and the gum.
- It is walked around each tooth, typically in six locations (mesiobuccal, midbuccal, distobuccal, mesiolingual, midlingual, and distolingual).
- The depth is measured from the gingival margin to the base of the pocket.
b. Interpretation of Probing Depths
- 1–3 mm: Healthy sulcus; no treatment needed.
- 4 mm: Mild periodontal involvement; may indicate gingivitis or early periodontitis.
- 5–6 mm: Moderate pocket depth; often suggests moderate periodontitis.
- 7 mm or more: Severe periodontitis; indicates advanced attachment and bone loss.
Probing depths greater than 4 mm are considered periodontal pockets and warrant further investigation and often intervention.
c. Factors Affecting Probing Accuracy
- Probe angulation and pressure can affect readings.
- Presence of calculus may impede full penetration.
- Inflammation can result in false deep readings due to soft tissue edema.
- Operator experience and consistency are essential for reliable measurements.
2. Clinical Attachment Level (CAL)
While probing depth measures from the gingival margin to the base of the pocket, Clinical Attachment Level (CAL) provides a more accurate measure of attachment loss by measuring from the cementoenamel junction (CEJ) to the base of the pocket.
a. Importance of CAL
- Reflects true loss of periodontal support.
- Helps distinguish between pseudopockets (from gingival overgrowth) and true pockets (from attachment loss).
- CAL is used in staging and grading periodontitis.
b. Calculation of CAL
- If gingival margin is at CEJ: CAL = Probing Depth
- If recession is present: CAL = Probing Depth + Recession
- If gingival overgrowth: CAL = Probing Depth – Distance from CEJ to gingival margin
3. Bleeding on Probing (BOP)
Bleeding on Probing is a key indicator of active inflammation in the periodontal tissues.
- Recorded immediately after probing each site.
- Indicates ulceration of the pocket lining and ongoing infection.
- Presence of BOP correlates with disease activity and risk of progression.
- Absence of BOP over time suggests disease stability or effective treatment.
Chronic bleeding also reflects systemic vascular changes and may be more pronounced in patients with underlying conditions like diabetes or blood disorders.
4. Suppuration (Pus Discharge)
Suppuration, or pus exudation, from the periodontal pocket indicates purulent infection and is often associated with:
- Advanced periodontitis
- Deep pockets with necrotic tissue
- Periodontal abscess formation
Though not always present, suppuration is a clear sign of active bacterial infection and often necessitates immediate antimicrobial or surgical intervention.
5. Tooth Mobility Assessment
Tooth mobility is assessed manually or with specialized instruments (e.g., Miller Index). It reflects the integrity of the periodontal ligament and bone:
- Class I: Slight mobility (up to 1 mm in horizontal direction)
- Class II: Moderate mobility (more than 1 mm)
- Class III: Severe mobility (movement in all directions, including vertical)
Mobility often increases as periodontal pockets deepen and alveolar bone is lost.
6. Radiographic Examination
Dental radiographs are an essential tool for visualizing alveolar bone levels and evaluating the structural impact of periodontal disease.
a. Types of Radiographs Used
- Periapical radiographs: Provide detailed images of individual teeth and surrounding bone.
- Bitewing radiographs: Useful for detecting horizontal bone loss, especially in posterior teeth.
- Panoramic radiographs: Offer an overall view but are less detailed for periodontal assessment.
- Cone Beam Computed Tomography (CBCT): Advanced 3D imaging for complex or surgical cases.
b. Radiographic Indicators of Periodontal Pockets
- Loss of crestal bone height.
- Angular (vertical) bone defects.
- Furcation involvement in multi-rooted teeth.
- Widening of periodontal ligament space.
Radiographs cannot directly visualize pocket depth, but they provide critical context when used alongside clinical probing.
7. Periodontal Charting
Comprehensive periodontal charting documents all clinical findings in a systematic format. It typically includes:
- Probing depths at six points per tooth.
- Clinical attachment levels.
- Bleeding on probing.
- Tooth mobility.
- Furcation involvement (in multi-rooted teeth).
- Recession levels.
- Presence of plaque and calculus.
This chart serves as a baseline for diagnosis, treatment planning, and monitoring over time. It also enhances communication between general dentists and periodontists and ensures continuity of care.
8. Furcation Involvement Evaluation
Furcation involvement occurs when periodontal pockets extend into the area between the roots of multi-rooted teeth (e.g., molars).
a. Classification (Glickman’s Classification)
- Grade I: Incipient furcation involvement; slight bone loss.
- Grade II: Partial bone loss; probe can enter the furcation but not pass through.
- Grade III: Complete bone loss; probe can pass through but not visible.
- Grade IV: Same as Grade III but with visible furcation due to gingival recession.
Furcation involvement complicates cleaning and treatment, and often requires specialized surgical management.
9. Microbiological and Diagnostic Testing (Advanced Cases)
In some advanced or refractory cases, microbiological testing may be performed to identify the specific bacterial species involved. This can help tailor antibiotic therapy. Common techniques include:
- DNA probe analysis
- Polymerase Chain Reaction (PCR)
- Bacterial cultures
Additional diagnostic tests may include:
- Host-response markers (e.g., interleukins, prostaglandins)
- Salivary diagnostics to assess inflammatory mediators
- Genetic susceptibility testing for predisposition to periodontitis
These tools are typically used in specialized periodontal or research settings.
10. Staging and Grading of Periodontitis
As part of the diagnostic process, the 2017 AAP/EFP classification system is used to determine the Stage and Grade of the disease:
a. Staging (based on severity and complexity)
- Stage I: Initial periodontitis (1–2 mm attachment loss)
- Stage II: Moderate periodontitis (3–4 mm loss)
- Stage III: Severe periodontitis with potential tooth loss (≥5 mm)
- Stage IV: Advanced periodontitis with loss of dentition and function
b. Grading (based on rate of progression and risk factors)
- Grade A: Slow progression
- Grade B: Moderate progression (most common)
- Grade C: Rapid progression, often with systemic involvement or risk factors (e.g., smoking, diabetes)
This classification helps guide treatment intensity and predict long-term outcomes.
Importance of Early Diagnosis
Early detection of periodontal pockets is vital for:
- Preventing irreversible bone loss.
- Reducing the risk of systemic complications.
- Preserving natural teeth.
- Avoiding extensive, costly treatments later on.
Routine periodontal exams are recommended at least once a year—or more frequently for patients with risk factors.
Summary of Diagnostic Tools and Indicators
| Diagnostic Method | Purpose |
|---|---|
| Periodontal probing | Measures pocket depth, identifies inflammation |
| Clinical attachment level | Assesses true attachment loss |
| Bleeding on probing (BOP) | Indicates active inflammation |
| Radiographs | Evaluates bone levels and architecture |
| Tooth mobility assessment | Gauges loss of support |
| Furcation involvement check | Determines root involvement in multi-rooted teeth |
| Periodontal charting | Comprehensive documentation of findings |
| Microbial testing (optional) | Identifies pathogenic bacteria, aids in targeted therapy |
| Salivary/genetic testing | Evaluates host response and susceptibility |
Treatment of Periodontal Pockets
The treatment of periodontal pockets is aimed at eliminating infection, halting disease progression, reducing pocket depth, and ideally restoring lost periodontal structures. Effective therapy must address both local bacterial factors and systemic contributing elements (e.g., diabetes, smoking). Treatment is typically tailored to the severity and extent of periodontal damage, the depth of the pockets, and the patient’s overall health and compliance.
Periodontal treatment is commonly divided into non-surgical (initial or Phase I therapy) and surgical (corrective or Phase II therapy), often followed by a maintenance phase (Phase IV).
1. Non-Surgical Treatment (Initial Therapy)
Non-surgical therapy is the first line of treatment for most cases of periodontal pockets. The goal is to reduce the bacterial load and inflammation without surgical intervention. This phase is sometimes sufficient, especially for mild to moderate periodontal pockets (4–5 mm).
a. Scaling and Root Planing (SRP)
Scaling removes plaque and calculus (tartar) from above and below the gumline. Root planing smooths the tooth root to discourage further plaque buildup and allow the gum tissue to reattach.
- Typically performed under local anesthesia.
- May be done quadrant-by-quadrant over multiple visits.
- Results in reduced inflammation, decreased pocket depth, and clinical attachment gain.
- Follow-up reevaluation is essential after 4–6 weeks to assess pocket response.
b. Local Antimicrobial Therapy
Antimicrobials can be applied directly into the pocket as an adjunct to SRP. These include:
- Chlorhexidine chips (PerioChip)
- Doxycycline gel (Atridox)
- Minocycline microspheres (Arestin)
These agents suppress bacterial activity for extended periods and can promote pocket reduction in sites not fully resolved by mechanical debridement.
c. Systemic Antibiotic Therapy
In certain cases—especially generalized aggressive periodontitis or when deep pockets are widespread—systemic antibiotics may be prescribed. Common regimens include:
- Amoxicillin + Metronidazole
- Clindamycin
- Doxycycline
However, systemic antibiotics are typically reserved for refractory or advanced cases to avoid resistance and systemic side effects.
d. Host Modulation Therapy (HMT)
Host modulation aims to control the body’s response to bacterial insult rather than the bacteria themselves. A common FDA-approved drug is:
Sub-antimicrobial dose doxycycline (Periostat): Inhibits matrix metalloproteinases (MMPs) involved in collagen destruction.
It is used in conjunction with SRP for moderate to severe chronic periodontitis.
e. Laser-Assisted Therapy
Lasers, such as diode, Nd:YAG, or erbium lasers, are used to:
- Decontaminate periodontal pockets.
- Remove inflamed epithelium.
- Promote coagulation and healing.
Laser-Assisted New Attachment Procedure (LANAP) is an FDA-cleared protocol that may provide reduced pocket depth and tissue regeneration with minimal invasion.
f. Oral Hygiene Education and Behavioral Modifications
Patients must be educated about:
- Effective brushing and interdental cleaning techniques.
- Antimicrobial mouth rinses (e.g., chlorhexidine gluconate).
- Tobacco cessation counseling.
- Nutritional support to promote healing.
Patient motivation and compliance are critical for successful long-term results.
2. Surgical Treatment (Corrective Therapy)
When non-surgical approaches are insufficient (e.g., persistent deep pockets ≥5 mm, vertical bone loss, furcation involvement), surgical intervention becomes necessary to:
- Access deeper deposits.
- Reshape or regenerate tissues.
- Reduce pocket depth for easier maintenance.
a. Flap Surgery (Open Flap Debridement)
In this procedure, the gum is lifted away from the tooth to allow better access to the root surfaces and bone. After cleaning and reshaping:
- The flap is repositioned and sutured in a tighter configuration to reduce pocket depth.
- Healing typically occurs within 7–10 days.
- Results in improved access for long-term maintenance.
b. Osseous Surgery
Also known as osseous recontouring or resective surgery, this procedure:
- Removes irregular bone defects and bony ledges.
- Reduces pocket depth by recontouring the supporting bone.
- Often performed in conjunction with flap surgery.
This approach is best suited for horizontal bone loss and when regeneration is not feasible.
3. Regenerative Periodontal Therapy
For certain cases—especially vertical or infrabony defects—the goal is not just pocket reduction, but true regeneration of the periodontium (bone, periodontal ligament, and cementum).
a. Bone Grafting
Bone grafts are used to fill vertical bone defects. Types include:
- Autografts: From the patient’s own body.
- Allografts: From human donors (e.g., demineralized freeze-dried bone).
- Xenografts: From animals, usually bovine-derived.
- Alloplasts: Synthetic bone substitutes.
Bone grafts act as scaffolds and stimulate new bone formation.
b. Guided Tissue Regeneration (GTR)
A barrier membrane is placed between the gum and the bone defect to:
- Prevent fast-growing epithelial cells from occupying the defect.
- Allow slower-growing periodontal ligament and bone cells to regenerate.
This method is effective for deep, localized infrabony defects and furcation areas.
c. Enamel Matrix Derivative (EMD)
A biologically active gel derived from developing tooth enamel (e.g., Emdogain) is applied to the root surface to stimulate:
- Formation of new cementum.
- Periodontal ligament regeneration.
- Alveolar bone regrowth.
d. Platelet-Rich Plasma (PRP) or Platelet-Rich Fibrin (PRF)
These biologic agents are derived from the patient’s blood and rich in growth factors:
- Accelerate healing and regeneration.
- Can be combined with bone grafts or membranes.
- Improve clinical attachment and bone fill in advanced defects.
4. Treatment of Furcation Involvement
Furcation defects (in multi-rooted teeth) require specialized approaches:
- Root planing or tunnel preparation for Grade I or II furcations.
- Furcation plasty or root resection in advanced cases.
- GTR or bone grafting for select Class II defects.
Furcation-involved teeth are harder to clean and maintain, and treatment success is variable depending on the anatomy and depth.
5. Maintenance Phase (Supportive Periodontal Therapy)
Periodontal pockets, even after treatment, have a tendency to recur. Thus, patients must enter a supportive periodontal therapy (SPT) program, involving:
- Regular check-ups every 3–6 months.
- Professional cleanings with subgingival debridement.
- Reassessment of pocket depths, attachment levels, and inflammation.
- Reinforcement of home care techniques.
- Management of systemic conditions and risk factors.
SPT is the long-term success factor in periodontal therapy. Patients who adhere to maintenance have significantly lower rates of tooth loss and disease recurrence.
6. Adjunctive and Emerging Therapies
a. Probiotics
Oral probiotics (e.g., Lactobacillus reuteri) may help restore microbial balance and reduce pathogenic bacteria. Still under research, they may serve as adjuncts in future maintenance protocols.
b. Photodynamic Therapy
This uses light-sensitive dyes and low-level lasers to kill bacteria in periodontal pockets with minimal tissue damage.
c. Host-Derived Biomaterials
Research is exploring the use of stem cells, bioengineered scaffolds, and growth factor cocktails to achieve complete periodontal regeneration in the future.
Selecting the Right Treatment Approach
Treatment selection depends on multiple factors:
| Consideration | Treatment Approach |
|---|---|
| Pocket depth 4–5 mm | SRP + local antimicrobials |
| Pocket depth ≥6 mm | Flap surgery ± regenerative procedures |
| Vertical bone defects | GTR, bone grafts, biologics |
| Furcation involvement | Surgical debridement, tunneling, regeneration, or root resection |
| Generalized aggressive disease | Systemic antibiotics + host modulation |
| Medical compromise | Conservative care with enhanced maintenance |
Goals of Periodontal Pocket Treatment
The overarching goals of therapy include:
- Eliminate microbial infection.
- Arrest disease progression.
- Reduce or eliminate pocket depth.
- Promote reattachment or regeneration of tissues.
- Restore function and aesthetics.
- Maintain long-term stability through preventive care.
Prevention of Periodontal Pockets
Maintaining periodontal health requires a combination of personal and professional care:
1. Daily Oral Hygiene
- Brush at least twice daily using fluoride toothpaste.
- Floss daily to remove plaque between teeth.
- Consider water flossers or interdental brushes for additional cleaning.
2. Regular Dental Check-Ups
Professional cleanings every 6 months (or more frequently for high-risk individuals) are essential for early detection and management.
3. Healthy Diet
A diet rich in vitamins and minerals supports gum health. Avoid sugary snacks and acidic beverages that promote plaque formation.
4. Quit Smoking
Smoking cessation significantly reduces the risk of periodontal disease progression.
5. Manage Systemic Conditions
Diabetes and other chronic conditions should be well-managed to reduce periodontal risk.