
White blood cells (WBCs), also known as leukocytes, are the unsung heroes of the human immune system. Despite comprising only about 1% of the total blood volume in a healthy adult, they play a crucial role in defending the body against infections, foreign invaders, and even abnormal internal cells such as cancer. In this comprehensive article, we will delve into the complex and fascinating world of white blood cells, exploring their structure, types, functions, development, and the disorders that can affect them.
Table of Contents
ToggleOverview of White Blood Cells
White blood cells are a diverse group of immune cells found in the blood and lymphatic system. Unlike red blood cells, which carry oxygen, WBCs are primarily involved in immune defense. They are produced in the bone marrow and circulate through the bloodstream and lymphatic system, patrolling for pathogens and responding to signs of infection or injury.
Basic Characteristics
- Size: Typically 12–17 micrometers in diameter, larger than red blood cells.
- Lifespan: Ranges from hours to years, depending on the type.
- Nucleus: All WBCs have a nucleus, distinguishing them from red blood cells.
- Mobility: Capable of moving independently and squeezing through blood vessel walls to reach tissues (a process called diapedesis).
Classification of White Blood Cells
WBCs are broadly classified into granulocytes and agranulocytes, based on the presence or absence of granules in their cytoplasm.
Granulocytes
These cells contain granules in their cytoplasm and are named based on the staining characteristics of these granules.
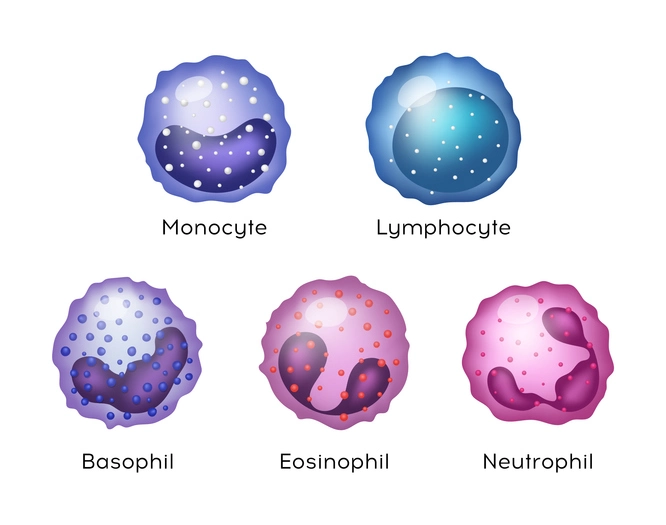
Neutrophils
- Most abundant WBC (50–70% of total).
- First responders to microbial infection.
- Specialized in phagocytosis – engulfing and digesting pathogens.
- Short-lived (a few hours to days).
- Important in the acute inflammatory response.
Eosinophils
- Comprise 1–4% of WBCs.
- Target parasites and are active in allergic reactions.
- Release enzymes that destroy parasitic invaders.
- Contribute to tissue damage in chronic allergies like asthma.
Basophils
- Least common (<1% of WBCs).
- Release histamine and other mediators of inflammation.
- Play a role in allergic and antigen response.
- Functionally similar to mast cells.
Agranulocytes
These lack visible cytoplasmic granules under a microscope.
Lymphocytes
- Second most abundant type (20–40%).
- Critical to adaptive immunity.
Divided into:
- B cells: Produce antibodies.
- T cells: Kill infected cells and coordinate immune responses.
- Natural Killer (NK) cells: Destroy virus-infected and tumor cells.
Monocytes
- Make up 2–8% of WBCs.
- Largest WBCs.
- Differentiate into macrophages or dendritic cells upon entering tissues.
- Act as phagocytes and antigen-presenting cells.
Functions of White Blood Cells
White blood cells are central to the body’s immune defense, performing a wide range of functions beyond simply attacking pathogens. These functions span across both the innate (non-specific) and adaptive (specific) arms of the immune system. Below is an in-depth exploration of the key roles WBCs play in maintaining homeostasis and defending the body:
- Phagocytosis: The Frontline Defense
- Antigen Presentation and Immune Activation
- Antibody Production (Humoral Immunity)
- Cellular Immunity: Killing Infected and Abnormal Cells
- Regulation of Immune Responses
- Inflammatory Response Coordination
- Allergic Reactions and Hypersensitivity
- Surveillance and Tumor Immunity
- Immune Memory and Vaccination
- Wound Healing and Tissue Repair
- Defense Against Parasites
- Detoxification and Clean-up Roles
Phagocytosis: The Frontline Defense
Phagocytosis is the process by which certain white blood cells, primarily neutrophils, monocytes, and macrophages, engulf and digest pathogens, dead cells, and debris.
Steps of Phagocytosis:
- Chemotaxis: WBCs are attracted to the site of infection by chemical signals (e.g., cytokines, complement proteins).
- Adherence: WBCs bind to the pathogen using receptors.
- Engulfment: The pathogen is engulfed into a phagosome.
- Digestion: The phagosome fuses with a lysosome, forming a phagolysosome where enzymes destroy the invader.
- Exocytosis: Residual material is expelled from the cell.
Example: When bacteria enter a wound, neutrophils are among the first responders and begin engulfing and destroying the microbes within minutes.
Antigen Presentation and Immune Activation
Some WBCs act as antigen-presenting cells (APCs) — primarily monocytes, macrophages, and dendritic cells.
- These cells process and display fragments of pathogens (antigens) on their surface using MHC class II molecules.
- They then migrate to lymph nodes to present these antigens to T helper cells, initiating the adaptive immune response.
Significance: This function bridges the innate and adaptive immune systems and is critical for immune memory and long-term protection.
Antibody Production (Humoral Immunity)
B lymphocytes (B cells) are responsible for producing antibodies, which are proteins that specifically bind to antigens.
Functions of Antibodies:
- Neutralization: Block pathogen attachment.
- Opsonization: Tag pathogens for destruction by phagocytes.
- Complement Activation: Trigger the complement cascade, leading to cell lysis.
- Agglutination: Clump pathogens together for easier removal.
Example: In a hepatitis B infection, B cells create antibodies that neutralize the virus and prevent it from infecting liver cells.
Cellular Immunity: Killing Infected and Abnormal Cells
T lymphocytes (T cells), especially cytotoxic T cells (CD8+ T cells) and natural killer (NK) cells, are involved in direct killing of infected or cancerous cells.
- Cytotoxic T Cells detect and destroy cells presenting foreign antigens via MHC class I molecules.
- NK Cells identify and kill cells lacking MHC class I (a common trick used by viruses and cancer).
Example: In a viral infection like influenza, cytotoxic T cells kill infected respiratory cells to contain the spread of the virus.
Regulation of Immune Responses
Regulatory T cells (Tregs) and various cytokines secreted by WBCs help modulate the intensity of immune responses and prevent autoimmune damage.
- Tregs suppress overactive immune cells and maintain tolerance to self-antigens.
- Helper T cells (CD4+ T cells) orchestrate immune responses by releasing cytokines that influence other WBCs, such as B cells and macrophages.
Importance: Prevents excessive immune activation, which could lead to conditions like autoimmune diseases or chronic inflammation.
Inflammatory Response Coordination
White blood cells are central players in initiating and resolving inflammation — the body’s response to injury or infection.
Key Actions in Inflammation:
- Basophils and mast cells release histamine, increasing blood flow and vessel permeability.
- Neutrophils flood the area to clear pathogens.
- Monocytes arrive later, mature into macrophages, and aid in tissue repair.
Phases of Inflammation:
- Initiation – Detection of injury or infection.
- Amplification – Recruitment and activation of WBCs.
- Resolution – Clearance of pathogens and repair of tissues.
Allergic Reactions and Hypersensitivity
Eosinophils, basophils, and mast cells play major roles in type I hypersensitivity reactions, such as allergies and asthma.
- They release histamines, leukotrienes, and other inflammatory mediators.
- These cause symptoms like swelling, itching, bronchoconstriction, and mucus secretion.
Example: In hay fever, exposure to pollen triggers mast cells and basophils to release histamine, leading to sneezing and watery eyes.
Surveillance and Tumor Immunity
WBCs, especially natural killer (NK) cells and cytotoxic T cells, continuously monitor the body for abnormal cells such as tumor cells.
- They can recognize “altered self” markers on the surface of transformed cells.
- This immune surveillance is critical in cancer prevention.
Application: Some immunotherapies enhance WBC tumor surveillance to treat cancers like melanoma or leukemia.
Immune Memory and Vaccination
Memory B cells and memory T cells are long-lived cells that “remember” specific pathogens after initial exposure.
- They provide faster and more robust responses upon re-infection.
- Vaccines exploit this mechanism by introducing harmless antigens to train WBCs without causing disease.
Example: After receiving the measles vaccine, memory cells ensure lifelong immunity in most people.
Wound Healing and Tissue Repair
After infection or injury, WBCs like macrophages help transition the body from inflammation to healing.
- Macrophages clear dead cells and secrete growth factors that stimulate tissue regeneration.
- They also interact with fibroblasts to aid in collagen production and scar formation.
Relevance: Chronic wounds, such as diabetic ulcers, often involve impaired WBC function.
Defense Against Parasites
Eosinophils are specialized in combating large parasites like helminths (worms), which are too big for phagocytosis.
- They release toxic granules and enzymes onto the parasite’s surface.
- IgE antibodies help eosinophils and mast cells recognize and attach to these invaders.
Example: Infections by Schistosoma or Ascaris worms see a spike in eosinophil levels (eosinophilia).
Detoxification and Clean-up Roles
White blood cells not only defend against infections but also help clean up:
- Dead or dying cells.
- Damaged tissue components.
- Toxins or foreign particles.
This “sanitation” role ensures the internal environment remains clean and stable.
White Blood Cell Formation (Leukopoiesis)
A. Hematopoietic Stem Cells
All blood cells originate from multipotent hematopoietic stem cells (HSCs) in the bone marrow.
B. Differentiation Pathways
- HSCs differentiate into either myeloid or lymphoid progenitor cells.
- Myeloid lineage gives rise to neutrophils, eosinophils, basophils, monocytes, and some dendritic cells.
- Lymphoid lineage gives rise to B cells, T cells, and NK cells.
C. Regulation
Controlled by cytokines such as:
Interleukins (e.g., IL-2, IL-6)
Granulocyte colony-stimulating factor (G-CSF)
Macrophage colony-stimulating factor (M-CSF)
White Blood Cell Count and Normal Ranges
A white blood cell count (WBC count) is a crucial clinical test that measures the number of white blood cells in a microliter (µL) of blood. This test is part of a complete blood count (CBC) and provides valuable insights into a person’s immune status, inflammatory responses, and potential underlying conditions such as infections, autoimmune diseases, and hematological cancers.
How the WBC Count is Measured
- Blood is drawn from a vein and sent to a laboratory.
- An automated hematology analyzer typically calculates the WBC count.
- In some cases, a manual differential count is performed by examining a stained blood smear under a microscope, especially when abnormalities are suspected.
Normal WBC Count Range
| Age Group | Normal WBC Count (cells/µL) |
|---|---|
| Adults | 4,000 – 11,000 |
| Children | 5,000 – 13,000 |
| Newborns | 9,000 – 30,000 |
Note: These values may slightly vary depending on the lab, methodology, and the population studied.
The total WBC count is broken down further into a differential count, which provides percentages or absolute counts of the five major WBC types:
- Neutrophils
- Lymphocytes
- Monocytes
- Eosinophils
- Basophils
Each type has its own reference range and clinical significance.
Elevated WBC Count (Leukocytosis)
Leukocytosis refers to an abnormally high WBC count — typically above 11,000 cells/µL. It’s not a disease itself, but rather a sign of an underlying condition.
Common Causes of Leukocytosis:
- Infections (especially bacterial)
- Inflammation (autoimmune diseases like rheumatoid arthritis)
- Leukemia and other blood cancers
- Stress response (physical or emotional stress, trauma, burns)
- Allergies or asthma
- Smoking
- Medications (e.g., corticosteroids, epinephrine)
- Pregnancy and childbirth
Types of Leukocytosis by Cell Type:
- Neutrophilia: Most common; associated with bacterial infections, inflammation.
- Lymphocytosis: Often viral (e.g., mononucleosis, hepatitis).
- Monocytosis: Seen in tuberculosis, chronic inflammation.
- Eosinophilia: Allergic reactions, parasitic infections.
- Basophilia: Rare; may indicate myeloproliferative disorders.
Low WBC Count (Leukopenia)
Leukopenia is defined as a WBC count below 4,000 cells/µL. It may impair the body’s ability to fight infections and often requires further investigation.
Common Causes of Leukopenia:
- Viral infections (e.g., HIV, hepatitis, influenza)
- Bone marrow suppression (e.g., chemotherapy, radiation therapy)
- Autoimmune diseases (e.g., lupus)
- Aplastic anemia
- Malnutrition (especially deficiency in B12, folate, copper)
- Certain medications (e.g., anticonvulsants, antipsychotics, antibiotics)
- Sepsis (can lead to immune exhaustion and drop in WBCs)
- Congenital immunodeficiencies
WBC Differential: Normal Ranges and Interpretations
| WBC Type | % of Total WBCs | Absolute Range (cells/µL) | Key Role |
|---|---|---|---|
| Neutrophils | 50–70% | 2,000–7,000 | Phagocytosis, first-line defense |
| Lymphocytes | 20–40% | 1,000–4,000 | Adaptive immunity, antibody production |
| Monocytes | 2–8% | 100–800 | Phagocytosis, antigen presentation |
| Eosinophils | 1–4% | 50–500 | Allergic reactions, parasite defense |
| Basophils | 0.1–1% | 25–100 | Release of histamine, allergy involvement |
Clinical Relevance of WBC Count
WBC counts are often used in the diagnostic process and monitoring of treatment. Here’s how:
Diagnosis
- High WBC + fever + symptoms → likely infection.
- Low WBC + fatigue + bleeding → consider bone marrow suppression or leukemia.
- WBC changes with specific cell line elevations help narrow down the cause.
Treatment Monitoring
- Chemotherapy patients have regular WBC checks to assess immune competence.
- Immunosuppressive therapy (e.g., in organ transplant) requires WBC monitoring to avoid infections.
- Post-infection: WBC normalization is a sign of recovery.
WBC Count and COVID-19
In the context of COVID-19:
- Lymphopenia (low lymphocytes) was commonly observed in moderate to severe cases.
- A high neutrophil to lymphocyte ratio (NLR) has been used as a prognostic marker, indicating worse outcomes.
Fun Fact: Diurnal Variation of WBCs
Did you know your WBC count can vary throughout the day?
- It’s often lower in the morning and higher in the evening.
- Physical activity, emotional stress, and even meals can transiently affect WBC levels.
When Should You Be Concerned?
A single abnormal WBC count doesn’t always indicate a problem. Temporary changes can occur due to:
- Minor infections
- Stress
- Dehydration
- Menstrual cycles
However, persistent abnormal values, especially with symptoms like fatigue, fever, frequent infections, bruising, or unexplained weight loss, warrant further testing.
Summary Table
| Term | Meaning | WBC Range | Common Causes |
|---|---|---|---|
| Leukocytosis | High WBC count | >11,000/µL | Infection, inflammation, leukemia |
| Leukopenia | Low WBC count | <4,000/µL | Viral infections, chemo, lupus |
| Neutrophilia | High neutrophils | >7,000/µL | Bacterial infection, stress |
| Neutropenia | Low neutrophils | <1,500/µL | Bone marrow damage, sepsis |
| Lymphocytosis | High lymphocytes | >4,000/µL | Viral infection, leukemia |
| Lymphopenia | Low lymphocytes | <1,000/µL | HIV, steroids, autoimmune disease |
Disorders Related to White Blood Cells
White blood cells are essential for immune defense, but like any system in the body, they are vulnerable to malfunction, infection, overproduction, and destruction.
Quantitative WBC Disorders
These involve either an increase or decrease in WBC counts.
Leukocytosis (High WBC Count)
Leukocytosis is an elevated white blood cell count, generally >11,000 cells/µL. It is usually a response, not a disease itself.
Common Causes:
- Infections (especially bacterial)
- Chronic inflammation
- Physical or emotional stress
- Leukemias and lymphomas
- Tissue damage (e.g., burns, trauma)
- Post-surgery
- Smoking or obesity
Types by WBC Subtype:
- Neutrophilia – Seen in bacterial infections, tissue necrosis.
- Lymphocytosis – Viral infections (e.g., Epstein-Barr Virus).
- Monocytosis – Chronic infections (e.g., tuberculosis).
- Eosinophilia – Allergies, parasitic infections.
- Basophilia – Myeloproliferative diseases (e.g., CML).
Leukopenia (Low WBC Count)
Leukopenia is a reduction in total WBCs, usually <4,000 cells/µL, making the body more susceptible to infections.
Causes:
- Viral infections (e.g., HIV, hepatitis)
- Autoimmune diseases (e.g., lupus, rheumatoid arthritis)
- Bone marrow suppression (e.g., radiation, chemotherapy)
- Aplastic anemia
- Drugs (e.g., clozapine, methotrexate)
- Malnutrition
Neutropenia (low neutrophils):
- <1,500 cells/µL is considered neutropenia.
- <500 cells/µL is severe neutropenia and a medical emergency.
Qualitative WBC Disorders
In these conditions, WBCs may be present in normal numbers but fail to function properly.
Chronic Granulomatous Disease (CGD)
- A rare inherited disorder where phagocytes can’t kill certain bacteria and fungi due to defective enzymes.
- Results in frequent infections and granuloma formation.
- Diagnosed using nitroblue tetrazolium (NBT) test or genetic testing.
- Managed with antibiotics, antifungals, and sometimes bone marrow transplant.
Chediak-Higashi Syndrome
- A rare autosomal recessive disorder with defective lysosomal trafficking.
- Leads to giant granules in WBCs and impaired phagocytosis.
- Symptoms include recurrent infections, albinism, and neurologic issues.
- Often fatal in childhood if untreated.
Leukocyte Adhesion Deficiency (LAD)
- A genetic disorder where WBCs cannot adhere to blood vessel walls to migrate to infection sites.
- Leads to delayed wound healing, severe bacterial infections, and absence of pus despite infection.
- Treatment: Bone marrow transplant is often curative.
Hematologic Malignancies (Blood Cancers)
These are cancers of the bone marrow and lymphatic system that affect WBC production and function.
Leukemia
A group of cancers affecting white blood cell precursors in the bone marrow, leading to overproduction of abnormal WBCs and bone marrow failure.
Types of Leukemia:
| Type | Description | Common in |
|---|---|---|
| ALL (Acute Lymphocytic Leukemia) | Rapid onset; affects lymphoid precursors | Children |
| AML (Acute Myeloid Leukemia) | Rapid onset; affects myeloid precursors | Adults |
| CLL (Chronic Lymphocytic Leukemia) | Slow-growing; affects mature lymphocytes | Elderly |
| CML (Chronic Myeloid Leukemia) | Linked to Philadelphia chromosome | Adults (30–60 yrs) |
Symptoms:
- Fatigue
- Easy bruising or bleeding
- Frequent infections
- Bone pain
- Weight loss
Treatment:
- Chemotherapy
- Radiation
- Targeted therapy (e.g., tyrosine kinase inhibitors for CML)
- Bone marrow/stem cell transplant
Lymphoma
Cancer of the lymphatic system, often affecting lymphocytes and lymph nodes.
Types:
- Hodgkin lymphoma – Characterized by Reed-Sternberg cells.
- Non-Hodgkin lymphoma (NHL) – A diverse group with various behaviors and treatments.
Symptoms:
- Painless lymph node swelling
- Night sweats
- Fever
- Unexplained weight loss
Autoimmune WBC Disorders
In these disorders, the immune system mistakenly attacks WBCs or uses WBCs to attack healthy tissues.
Systemic Lupus Erythematosus (SLE)
- Autoimmune disease where WBCs attack the body’s own tissues.
- May result in leukopenia, particularly lymphopenia.
- Symptoms: Fatigue, joint pain, skin rashes, kidney damage.
Rheumatoid Arthritis (RA)
- Rheumatoid Arthritis, chronic inflammatory disease affecting joints.
- WBCs invade joint tissues, releasing inflammatory cytokines.
- Can lead to elevated WBCs in synovial fluid but sometimes low counts in blood due to bone marrow effects or medications.
Autoimmune Neutropenia
- Antibodies destroy neutrophils.
- Can be congenital (in infants) or acquired (in adults).
- Treated with G-CSF (granulocyte colony-stimulating factor) to stimulate production.
Infectious Diseases Affecting WBCs
Some pathogens directly affect WBC numbers or function:
HIV/AIDS
- Destroys CD4+ T helper cells, a type of lymphocyte.
- Leads to lymphopenia and immunosuppression.
- Increased risk of opportunistic infections and certain cancers.
Epstein-Barr Virus (EBV) / Infectious Mononucleosis
- Causes lymphocytosis with atypical lymphocytes.
- Symptoms: Sore throat, fever, swollen lymph nodes, fatigue.
Sepsis
- A life-threatening infection that can cause neutropenia or leukocytosis, depending on severity and phase.
- Immune system becomes dysregulated, leading to organ failure and shock.
Drug-Induced WBC Disorders
Certain medications can suppress or stimulate WBC production:
| Medication Class | Effect on WBCs |
|---|---|
| Chemotherapy | Bone marrow suppression → neutropenia |
| Clozapine (antipsychotic) | Can cause agranulocytosis (dangerous drop in neutrophils) |
| Corticosteroids | Can cause transient leukocytosis |
| Antibiotics (e.g., sulfonamides) | May cause immune-mediated neutropenia |
Regular blood monitoring is crucial when patients are on such medications.
Summary: Common WBC Disorders and Features
| Disorder | WBC Count | WBC Type Affected | Common Symptoms | Key Treatment |
|---|---|---|---|---|
| Leukemia | High/Low | Immature WBCs | Fatigue, bleeding, infections | Chemo, BMT |
| Lymphoma | Normal/High | Lymphocytes | Swollen lymph nodes, night sweats | Chemo, radiation |
| Neutropenia | Low | Neutrophils | Fever, recurrent infections | G-CSF, antibiotics |
| Eosinophilia | High | Eosinophils | Asthma, rash, itching | Steroids, antiparasitics |
| HIV/AIDS | Low | T lymphocytes | Opportunistic infections | ART (antiretroviral therapy) |
| Autoimmune neutropenia | Low | Neutrophils | Fever, sores, ulcers | G-CSF, immunosuppressants |
Diagnostic Tools and Tests
White blood cell analysis is essential in evaluating the immune system, diagnosing hematological disorders, and monitoring infections, autoimmune diseases, and cancers. The testing spectrum ranges from basic blood tests to advanced molecular diagnostics.
Complete Blood Count (CBC)
The Complete Blood Count (CBC) is the foundational test for assessing WBCs.
What It Measures:
- Total WBC count
- Red blood cell count
- Hemoglobin
- Hematocrit
- Platelet count
- WBC differential (may be automated or manual)
Clinical Use:
- Detect infections, inflammation, leukemia, allergies, and immune suppression.
- A routine part of physical exams and pre-operative assessments.
WBC Differential Count
This test measures the percentage and absolute number of each type of white blood cell:
- Neutrophils
- Lymphocytes
- Monocytes
- Eosinophils
- Basophils
Types:
- Automated differential: Done by machines using light scatter and electrical impedance.
- Manual differential: A lab technician reviews a stained blood smear under a microscope to visually identify WBC types — especially useful for detecting immature or abnormal cells.
Clinical Clues:
- High neutrophils → likely bacterial infection
- High lymphocytes → often viral infection
- High eosinophils → allergy or parasitic infection
- Presence of blast cells → potential leukemia
Peripheral Blood Smear
A peripheral smear involves spreading a drop of blood on a glass slide, staining it (typically with Wright-Giemsa stain), and examining it under a microscope.
What It Shows:
- Morphology (size, shape, granulation) of WBCs.
- Presence of immature or abnormal cells (e.g., blasts, atypical lymphocytes).
- Insight into qualitative disorders of WBCs.
Clinical Use:
- Diagnosing leukemias, infections, anemia types, and malaria.
- Confirming findings from automated analyzers.
Bone Marrow Aspiration and Biopsy
These tests evaluate the source of WBC production – the bone marrow.
Indications:
- Unexplained leukopenia or leukocytosis
- Diagnosis of leukemia or lymphoma
- Investigation of pancytopenia (reduction in all blood cells)
Procedure:
- Performed under local anesthesia, usually from the posterior iliac crest (hip bone).
- Aspiration: Withdraws a liquid sample of marrow.
- Biopsy: Removes a core of marrow tissue for histological analysis.
What It Can Reveal:
- Cellularity (marrow activity level)
- Presence of malignancy (e.g., leukemia, myeloma)
- Fibrosis, infection, or infiltration by other diseases
Flow Cytometry
Flow cytometry uses lasers to analyze physical and chemical characteristics of WBCs in a fluid sample.
Key Applications:
- Immunophenotyping: Identifying specific markers (CD markers) on cells.
- Diagnosing leukemia and lymphoma subtypes.
- Evaluating immune deficiencies.
- Monitoring response to therapy (e.g., minimal residual disease in leukemia).
Example:
- Identifying CD19+ B cells or CD3+ T cells to determine immune profile.
- CD34+ cells in bone marrow – important for stem cell transplantation.
Cytogenetic Analysis and Karyotyping
These tests examine the chromosomes of WBCs, usually from bone marrow or blood samples.
Uses:
- Detecting chromosomal abnormalities (e.g., Philadelphia chromosome t(9;22) in chronic myeloid leukemia).
- Evaluating congenital syndromes with immune dysfunction.
Techniques:
- Conventional karyotyping: Visualizes whole chromosomes under a microscope.
- FISH (Fluorescence In Situ Hybridization): Uses fluorescent probes to detect specific DNA sequences.
- Array CGH (Comparative Genomic Hybridization): Detects DNA copy number changes.
Molecular Genetic Testing
These tests identify gene mutations, translocations, or clonal markers related to WBC disorders.
Techniques:
- PCR (Polymerase Chain Reaction): Amplifies specific DNA segments for mutation analysis.
- Next-Generation Sequencing (NGS): Offers a broader analysis of multiple genes at once.
- Gene panels: Target specific leukemia or immunodeficiency-related genes.
Conditions Detected:
- Acute leukemias (e.g., FLT3, NPM1 mutations)
- Chronic lymphocytic leukemia (IGHV mutation status)
- Inherited immunodeficiencies (e.g., SCID gene mutations)
Serological and Immunologic Tests
These tests detect antibodies, antigens, or immune system activity related to WBC function.
Examples:
- Antinuclear antibody (ANA) – for autoimmune diseases like lupus.
- HIV test – evaluates cause of lymphopenia.
- IgE levels – high in allergies and eosinophilic disorders.
- Complement levels – assess immune system deficiencies.
Leukocyte Function Tests
Specialized tests used to assess how well WBCs respond, move, engulf, and destroy pathogens.
Examples:
- Nitroblue Tetrazolium (NBT) Test – Screens for chronic granulomatous disease (tests neutrophil oxidative burst).
- Dihydrorhodamine (DHR) Assay – A more advanced test for neutrophil function.
- Chemotaxis Assay – Evaluates WBC movement toward a chemical signal.
- Phagocytosis Assay – Measures ability to engulf bacteria or particles.
These are especially useful in diagnosing primary immunodeficiencies.
Immunohistochemistry (IHC)
This test uses antibodies tagged with enzymes or fluorescent markers to detect specific cell surface or intracellular markers in tissue biopsies.
Use Cases:
- Distinguishing between types of lymphoma.
- Detecting abnormal WBCs in lymph nodes, bone marrow, or other tissues.
- Correlating WBC marker expression with prognosis (e.g., CD20 in B-cell lymphomas).
Imaging Tests
While not directly analyzing WBCs, imaging helps track effects of WBC-related diseases.
Common Imaging Techniques:
- X-rays: For bone involvement in leukemia.
- CT/MRI: To evaluate lymphadenopathy in lymphoma.
- PET scans: Assess metabolic activity in lymphomas and other WBC cancers.
Monitoring Tools for Therapy
When treating WBC disorders (like leukemia), specialized tools help monitor response to treatment and disease progression:
- Minimal Residual Disease (MRD) testing via flow cytometry or PCR.
- Serial CBCs to monitor blood cell recovery post-chemotherapy.
- Chimerism studies post bone marrow transplant to assess donor cell integration.
Summary Table: Key WBC Diagnostic Tools
| Test | What It Evaluates | Primary Use |
|---|---|---|
| CBC + Differential | Total & type-specific WBC count | Routine screening, infection, inflammation |
| Blood Smear | Cell morphology | Leukemia, infections, anemia |
| Bone Marrow Biopsy | Marrow function | Leukemia, aplastic anemia |
| Flow Cytometry | Cell surface markers | Leukemia, lymphoma, immunodeficiency |
| Karyotyping/FISH | Chromosomal abnormalities | Leukemia, congenital syndromes |
| PCR/NGS | Gene mutations | Leukemia, inherited diseases |
| NBT/DHR Test | Neutrophil function | CGD, immunodeficiency |
| Serology | Immune response & antibodies | Autoimmune disease, allergies |
| Imaging (CT, PET) | Disease location/spread | Lymphoma, bone metastasis |
Conclusion
White blood cells are vital defenders of the human body, forming an intricate and dynamic network capable of recognizing, responding to, and remembering countless threats. They are key players not only in everyday immune surveillance but also in the broader landscape of medicine, from cancer therapies to vaccine development.
Understanding WBCs allows for better diagnostics, more effective treatments, and the ability to harness the immune system in revolutionary ways. As research continues, we will likely discover even more about the complex interplay of these microscopic warriors and their role in health and disease.