
A stroke is a medical emergency that occurs when the blood supply to a part of the brain is interrupted or reduced, depriving brain tissue of oxygen and nutrients. Within minutes, brain cells begin to die. As one of the leading causes of death and long-term disability worldwide, stroke has profound implications for individuals, families, and health systems.
Despite its prevalence, stroke is often misunderstood. The signs may go unrecognized, the risk factors underestimated, and the critical window for treatment missed. This article provides an in-depth exploration of stroke, from its types and causes to prevention and recovery, aiming to raise awareness and promote proactive health behavior.
Table of Contents
ToggleWhat is a Stroke?
A stroke, also known as a cerebrovascular accident (CVA), is a medical condition that occurs when the blood supply to part of the brain is suddenly interrupted, leading to brain cell injury or death. This interruption deprives brain tissue of oxygen and nutrients, which are essential for the brain’s survival and function. Within minutes, brain cells in the affected area begin to malfunction, and without timely medical intervention, many of them die, resulting in potentially permanent neurological damage.
The brain is the control center of the body. It regulates essential bodily functions such as breathing, heart rate, movement, sensation, speech, and cognition. Since neurons (brain cells) do not regenerate as easily as cells in other parts of the body, any loss of brain function due to stroke can lead to lasting disabilities, such as difficulty speaking, walking, thinking, or even recognizing people or places.
Brain’s Dependency on Blood Flow
To understand stroke, it’s important to grasp how the brain relies on continuous blood flow. The brain is supplied by a complex system of arteries, including the carotid arteries in the neck and the vertebral arteries at the back of the head. These arteries branch out into smaller vessels, delivering oxygen-rich blood to every corner of the brain.
A stroke occurs when either:
- A blood vessel is blocked (ischemic stroke), or
- A blood vessel bursts (hemorrhagic stroke).
In either case, the result is the same: interruption of blood supply, leading to a “brain attack.”
Pathophysiology of a Stroke
At a cellular level, stroke causes a cascade of damaging events:
- Energy failure: Without blood flow, neurons cannot produce ATP (adenosine triphosphate), the molecule that powers cellular functions.
- Ion imbalance: Loss of ATP causes failure of sodium-potassium pumps, leading to cellular swelling and dysfunction.
- Glutamate toxicity: Excitatory neurotransmitters like glutamate accumulate, overexciting nearby neurons and causing damage.
- Inflammation and oxidative stress: Immune cells rush to the site, releasing substances that can further damage brain tissue.
- Cell death: Depending on the severity and duration of the stroke, cells die through necrosis or apoptosis (programmed cell death).
This damage expands outward from the original site, in what is known as the ischemic penumbra, the area surrounding the core infarct. With rapid treatment, some of this surrounding tissue may be salvaged.
Difference Between Stroke, TIA, and Aneurysm
It’s helpful to distinguish a stroke from conditions that may seem similar:
- Transient Ischemic Attack (TIA): Often referred to as a “mini-stroke,” a TIA results from a temporary blockage. It causes stroke-like symptoms that resolve within 24 hours (usually in minutes). Although the symptoms go away, TIAs are serious warning signs of a potential full stroke in the future.
- Brain Aneurysm: An aneurysm is a bulging, weak area in the wall of a blood vessel in the brain. It can lead to a hemorrhagic stroke if it ruptures. However, not all aneurysms burst—some remain asymptomatic for years.
Stroke as a Neurological Emergency
A stroke is considered a neurological emergency because:
- It occurs suddenly, often without warning.
- Every minute of delay results in the loss of approximately 1.9 million neurons.
- Time-sensitive treatments, like thrombolytic therapy or mechanical clot removal, are most effective within a narrow window (typically 3–4.5 hours for tPA, up to 24 hours for thrombectomy in selected cases).
The concept of “time is brain” underlines the urgency of stroke treatment.
Types of Stroke
Understanding the different types of stroke is essential for proper diagnosis, treatment, and prevention. Although all strokes result from disrupted blood flow to the brain, the underlying causes and mechanisms can vary significantly. These differences influence both the clinical presentation and the management strategy.
Broadly, strokes are categorized into three main types:
- Ischemic Stroke
- Hemorrhagic Stroke
- Transient Ischemic Attack (TIA)
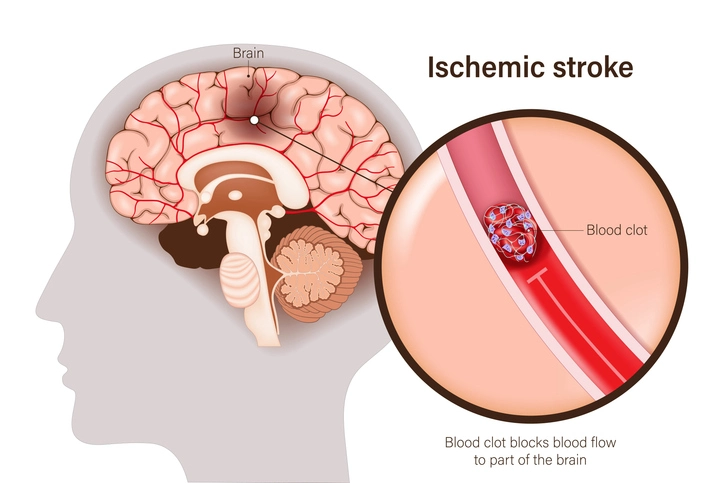
Ischemic Stroke (Blockage of Blood Flow)
Ischemic strokes are the most common type, accounting for approximately 87% of all strokes. They occur when a blood vessel supplying the brain becomes obstructed, cutting off oxygen and nutrients to part of the brain. Without this vital supply, brain cells begin to die within minutes.
Subtypes of Ischemic Stroke
a. Thrombotic Stroke
This type occurs when a blood clot (thrombus) forms directly in one of the arteries supplying the brain. Thrombotic strokes are often associated with atherosclerosis, a condition in which plaque builds up in the blood vessels over time.
- Large vessel thrombosis: Typically involves major arteries like the internal carotid or middle cerebral artery.
- Small vessel thrombosis (lacunar stroke): Affects small, deep arteries in the brain. Often linked to chronic hypertension and diabetes.
Symptoms: Depend on the area of the brain affected. Common signs include weakness on one side, speech problems, and visual disturbances.
b. Embolic Stroke
An embolic stroke happens when a blood clot or other debris forms in another part of the body (commonly the heart) and travels through the bloodstream to the brain, where it lodges in a narrower artery.
Common causes include:
- Atrial fibrillation (AFib) – Irregular heartbeat that can cause clot formation.
- Heart valve disease
- Endocarditis
- Fat or air embolism (rare)
Symptoms: Sudden onset, may occur during activity or rest. Often affects younger patients compared to thrombotic stroke.
Hemorrhagic Stroke (Bleeding in the Brain)
A hemorrhagic stroke occurs when a weakened blood vessel ruptures, causing bleeding either directly into the brain or into the surrounding space. Though less common (accounting for about 13% of strokes) hemorrhagic strokes tend to be more deadly and cause more severe disability.
Subtypes of Hemorrhagic Stroke
a. Intracerebral Hemorrhage (ICH)
This is the most common type of hemorrhagic stroke, caused by bleeding directly into the brain tissue due to the rupture of a blood vessel.
Causes:
- Chronic hypertension (most common)
- Trauma
- Arteriovenous malformations (AVMs)
- Blood-thinning medications (e.g., warfarin)
- Illicit drug use (e.g., cocaine, amphetamines)
Symptoms:
- Sudden headache
- Vomiting
- Decreased consciousness
- Focal neurological deficits (e.g., weakness, speech problems)
b. Subarachnoid Hemorrhage (SAH)
In a subarachnoid hemorrhage, bleeding occurs into the subarachnoid space, the area between the brain and the thin tissues covering it.
- Primary cause: Ruptured cerebral aneurysm.
- Other causes: AVMs, trauma, or bleeding disorders.
Symptoms:
- Sudden, severe “thunderclap” headache (often described as the worst headache of one’s life)
- Neck stiffness
- Light sensitivity
- Nausea and vomiting
- Loss of consciousness or seizure
SAH is a medical emergency and requires rapid intervention, often with surgical repair of the aneurysm or vascular abnormality.
Transient Ischemic Attack (TIA) – “Mini-Stroke”
A transient ischemic attack (TIA) is a temporary disruption of blood flow to the brain, spinal cord, or retina, typically lasting less than 24 hours (usually just a few minutes). Unlike other strokes, TIAs do not cause permanent brain damage, but they are a critical warning sign of an impending major stroke.
- Cause: Similar to ischemic stroke—often a small clot that temporarily blocks an artery but then dissolves or moves on.
- Symptoms: Identical to those of a full stroke—sudden weakness, speech difficulty, confusion, or vision problems—but they resolve completely.
- Prognosis: People who experience a TIA are at high risk of having a full ischemic stroke within days or weeks. Approximately 1 in 3 people who have a TIA will eventually have a stroke.
Management: A TIA warrants the same urgency as a full stroke, with thorough evaluation and preventive treatment (blood thinners, cholesterol-lowering drugs, or surgical interventions like carotid endarterectomy).
Other Stroke Classifications and Rare Types
Though most strokes fall into the three main categories, some specialized types exist based on cause, location, or underlying disease.
1. Cryptogenic Stroke
A stroke with no identified cause after comprehensive evaluation. Up to 30–40% of ischemic strokes may be cryptogenic. Further testing often includes long-term cardiac monitoring for undetected atrial fibrillation.
2. Brain Stem Stroke
A stroke occurring in the brain stem can impair vital functions such as breathing, heartbeat, and eye movement. It may also result in locked-in syndrome, where a person is conscious but unable to move or speak.
3. Watershed Stroke
These occur in areas of the brain that lie between major arteries (the “watershed” zones) and are particularly vulnerable during systemic hypoperfusion—often due to cardiac arrest, severe hypotension, or shock.
4. Cerebellar Stroke
Affects the cerebellum, which controls balance and coordination. Symptoms may include dizziness, nausea, unsteadiness, and difficulty walking. It is often misdiagnosed due to lack of typical stroke signs.
Comparison Table: Types of Stroke
| Type | Cause | Prevalence | Onset | Typical Symptoms | Reversibility |
|---|---|---|---|---|---|
| Ischemic Stroke | Blocked artery | ~87% | Sudden | Weakness, speech trouble, numbness | May recover with prompt treatment |
| Hemorrhagic Stroke | Burst blood vessel | ~13% | Sudden | Severe headache, vomiting, coma | Often permanent damage |
| Transient Ischemic Attack | Temporary blockage (resolves) | Warning sign | Sudden | Same as stroke but brief and reversible |
Risk Factors for Stroke
A risk factor is any attribute, condition, or behavior that increases the likelihood of developing a disease—in this case, stroke. Stroke is not entirely random; in fact, it is largely preventable, with up to 80% of strokes attributed to modifiable risk factors. Understanding these risk factors is crucial for prevention, early detection, and long-term management.
Risk factors are generally divided into two categories:
- Modifiable Risk Factors – Things you can change or manage
- Non-Modifiable Risk Factors – Things you cannot change (but should still be aware of)
Modifiable Risk Factors
These are the factors that individuals can control or manage through lifestyle changes, medical intervention, or both. Targeting these significantly reduces the likelihood of having a stroke.
1. Hypertension (High Blood Pressure)
- Most important risk factor for both ischemic and hemorrhagic strokes.
- Sustained high blood pressure can damage arterial walls, make them less elastic, and promote atherosclerosis (plaque buildup).
- It can also cause arteries to rupture, leading to bleeding in the brain.
Management:
- Regular blood pressure monitoring
- Medication adherence (ACE inhibitors, beta-blockers, diuretics)
- Reducing salt intake
- Physical activity
2. Diabetes Mellitus
- People with diabetes are 1.5 to 2 times more likely to have a stroke.
- High blood glucose levels over time can damage blood vessels and nerves, increasing the risk of both clot formation and hemorrhage.
- Diabetes is closely linked with other stroke risk factors like obesity, hypertension, and dyslipidemia.
Management:
- Maintain HbA1c levels <7%
- Monitor glucose regularly
- Use medications such as metformin or insulin as prescribed
- Adopt a diabetic-friendly diet
3. High Cholesterol (Dyslipidemia)
- Elevated levels of LDL (low-density lipoprotein) cholesterol contribute to plaque buildup in arteries, leading to atherosclerosis.
- This narrows or blocks arteries, especially those leading to the brain.
Management:
- Statins (e.g., atorvastatin, rosuvastatin)
- Diet rich in fiber, fruits, and vegetables
- Reduced intake of trans and saturated fats
- Routine lipid profile checks
4. Smoking
- Smoking doubles the risk of stroke.
- It damages blood vessels, reduces oxygen in the blood, increases clot formation, and accelerates atherosclerosis.
- Secondhand smoke is also a risk.
Management:
- Complete smoking cessation
- Nicotine replacement therapy (patches, gums)
- Behavioral counseling
- Support groups or cessation programs
5. Obesity and Overweight
- Increases the likelihood of high blood pressure, diabetes, and heart disease—all major stroke risk factors.
- Also associated with a sedentary lifestyle, poor diet, and metabolic syndrome.
Management:
- Aim for a healthy BMI (18.5–24.9)
- Nutritional counseling
- Regular physical activity (at least 150 minutes of moderate-intensity exercise per week)
- Weight-loss medications or bariatric surgery (in severe cases)
6. Physical Inactivity
- A sedentary lifestyle contributes to obesity, hypertension, and insulin resistance.
- Even moderate activity like walking, swimming, or gardening can reduce stroke risk.
Recommendations:
- At least 30 minutes of physical activity, five days a week
- Incorporate both cardio and strength training
7. Unhealthy Diet
Diets high in sodium, saturated fats, sugar, and processed foods contribute to obesity, high cholesterol, and hypertension.
Stroke-preventive diets include:
- DASH diet (Dietary Approaches to Stop Hypertension)
- Mediterranean diet (rich in fruits, vegetables, whole grains, fish, and olive oil)
8. Excessive Alcohol Intake
- Binge drinking and chronic alcoholism increase blood pressure and can lead to atrial fibrillation.
- Heavy alcohol use is particularly associated with hemorrhagic strokes.
Guidelines:
- Men: ≤2 standard drinks/day
- Women: ≤1 standard drink/day
- Complete abstinence in high-risk individuals
9. Atrial Fibrillation (AFib) and Other Heart Conditions
- AFib is an irregular heart rhythm that causes blood to pool and clot in the heart.
- These clots can travel to the brain and cause embolic strokes.
- Other heart conditions like heart failure, valve disease, and cardiomyopathy also increase risk.
Management:
- Anticoagulant therapy (e.g., warfarin, DOACs)
- Heart rate and rhythm control (beta-blockers, antiarrhythmics)
- Cardiac ablation in selected cases
10. Illicit Drug Use
- Cocaine, amphetamines, and other stimulants can elevate blood pressure, constrict blood vessels, and provoke hemorrhagic strokes.
- Drugs may also lead to cardiac arrhythmias, contributing to embolic strokes.
Prevention:
Substance use counseling and rehabilitation programs
Non-Modifiable Risk Factors
These are factors that cannot be changed but must be acknowledged and monitored, especially when combined with modifiable risks.
1. Age
- Stroke risk doubles each decade after age 55.
- However, strokes are increasingly affecting younger adults, especially due to rising rates of diabetes, obesity, and smoking.
2. Sex (Gender)
- Men have a higher stroke incidence at younger ages.
- Women, especially older women, have a higher lifetime stroke risk and worse outcomes.
- Pregnancy, oral contraceptive use, and hormone replacement therapy can increase risk in women.
3. Race and Ethnicity
- African Americans have a higher risk of stroke and are more likely to die from stroke than White individuals.
- Hispanics, Native Americans, and Asian Americans also face increased risks.
- Contributing factors include socioeconomic disparities, access to care, and higher prevalence of hypertension and diabetes.
4. Family History and Genetics
- A family history of stroke or cardiovascular disease increases your risk.
- Genetic disorders like sickle cell disease, CADASIL, and hypercoagulable states also raise stroke risk.
5. Previous Stroke or TIA
- Having had a stroke or TIA greatly increases the chance of having another.
- Recurrent strokes are often more disabling or fatal.
Secondary prevention becomes critical: lifestyle changes, medications, and sometimes surgical interventions (like carotid artery surgery or stenting).
Emerging and Less-Recognized Risk Factors
1. Sleep Apnea
- Obstructive sleep apnea is linked to increased blood pressure, atrial fibrillation, and systemic inflammation.
- Often undiagnosed and undertreated.
2. Chronic Inflammation
Conditions like rheumatoid arthritis, lupus, and inflammatory bowel disease can increase stroke risk.
3. Psychological Stress and Depression
Chronic stress and depression may contribute to unhealthy behaviors and physiological changes like inflammation and hypertension.
4. COVID-19 and Infections
- The SARS-CoV-2 virus has been associated with blood clotting abnormalities and increased risk of stroke, even in young individuals.
- Other infections (e.g., HIV, syphilis, varicella) can also contribute to stroke, particularly in immunocompromised people.
Signs and Symptoms of Stroke
Recognizing the signs and symptoms of stroke is vital, as every minute of delay in treatment increases the risk of irreversible brain damage. Stroke presentations can vary widely depending on the type of stroke, its location in the brain, and the extent of tissue affected. Below is an in-depth look at the common, less common, and atypical presentations of stroke.
1. Sudden Onset and Focal Neurological Deficits
Most strokes come on suddenly, with symptoms peaking within minutes. Because strokes interrupt blood flow to a specific brain region, the deficits are often focal—that is, they correspond to the functions governed by that brain area.
a. Motor Weakness or Paralysis
- Hemiparesis (weakness on one side of the body) or hemiplegia (complete paralysis).
- Often affects the face, arm, and leg on the same side.
- Facial droop may be subtle: one corner of the mouth may sag, or the eye may not close completely.
b. Sensory Disturbances
- Numbness, tingling, or loss of sensation, usually on one side.
- Patients may describe limbs as feeling “dead” or “numb.”
c. Visual Deficits
- Homonymous hemianopia: loss of the same half of the visual field in both eyes (e.g., left visual field).
- Diplopia (double vision) if cranial nerves controlling eye movement are involved.
d. Speech and Language Impairment
Aphasia: impairment in language production or comprehension.
Broca’s (expressive) aphasia: non-fluent speech, good comprehension.
Wernicke’s (receptive) aphasia: fluent but nonsensical speech, poor comprehension.
Dysarthria: slurred or garbled speech due to muscle weakness.
e. Coordination and Ataxia
- Cerebellar strokes present with difficulty walking, staggering, or inability to coordinate arm movements (dysmetria).
- Patients may describe a “drunken” gait or feel unsteady on their feet.
2. The FAST Acronym and Beyond
To aid rapid recognition, many health organizations promote the FAST mnemonic:
- Face drooping
- Arm weakness
- Speech difficulty
- Time to call emergency services
However, FAST focuses primarily on anterior circulation ischemic strokes. Other critical symptoms can be missed if only FAST is used.
3. Posterior Circulation and Brainstem Presentations
Strokes in the posterior circulation (vertebral and basilar arteries) or brainstem can produce less intuitive symptoms:
- Vertigo or sudden severe dizziness
- Nausea and vomiting
- Dysphagia (difficulty swallowing) and dysarthria
- Diplopia from cranial nerve involvement
- Drop attacks: sudden falls without loss of consciousness
- Locked-in syndrome: the patient is conscious and can think normally but cannot move or speak, only able to blink or move the eyes vertically.
Because these presentations can mimic inner-ear or gastrointestinal conditions, they are often misdiagnosed, delaying treatment.
4. Headache and Seizures
- Severe headache is more common in hemorrhagic strokes, especially subarachnoid hemorrhage (“thunderclap headache”).
- Seizures may occur at stroke onset or during recovery, particularly with cortical hemorrhages.
5. Transient and “Silent” Strokes
- Transient Ischemic Attacks (TIAs) produce stroke-like symptoms that resolve within 24 hours (often minutes). Though symptoms disappear, TIAs are urgent warning signs of a future stroke risk.
- Silent strokes cause brain tissue damage without overt symptoms. They are often discovered incidentally on MRI and are linked to cognitive decline, gait disturbances, and increased risk of symptomatic stroke.
6. Stroke Severity and Clinical Scales
Clinicians use quantifiable scales to assess stroke severity, predict outcomes, and guide treatment:
- NIH Stroke Scale (NIHSS): evaluates consciousness, vision, motor function, ataxia, sensory function, language, and attention. Scores range from 0 (no deficit) to 42 (severe stroke).
- Glasgow Coma Scale (GCS): sometimes used in hemorrhagic stroke to assess consciousness level.
A higher NIHSS correlates with larger infarcts, greater disability, and less likelihood of good recovery, but even patients with high scores may benefit from aggressive intervention if within treatment windows.
7. Atypical and Mimicking Conditions
Some conditions can mimic stroke or present atypically, complicating diagnosis:
- Hypoglycemia: low blood sugar can cause weakness, confusion, and slurred speech. Always check a finger-stick glucose.
- Migraine with aura: can produce transient neurological symptoms like visual changes or paresthesias.
- Seizure with postictal paralysis (Todd’s palsy): transient weakness after a seizure.
- Infections (e.g., encephalitis) or tumors can present with focal deficits but have a more gradual onset.
8. Importance of Public Awareness
Because stroke symptoms vary so widely, public education campaigns emphasize:
- Recognizing non-FAST signs (e.g., sudden dizziness, severe headache, vision changes).
- Calling emergency services immediately if any sudden neurological symptom occurs.
- Not waiting to see if symptoms improve.
Diagnosis of Stroke
Accurate and rapid diagnosis is crucial in stroke care because the effectiveness of treatment depends heavily on how quickly the type and severity of the stroke are identified. A successful diagnosis involves a systematic approach: clinical evaluation, imaging studies, laboratory tests, and cardiac assessments. This comprehensive evaluation not only confirms the presence of a stroke but also distinguishes between ischemic and hemorrhagic stroke, identifies the stroke subtype, determines the location and extent of brain damage, and uncovers the underlying cause, all of which are critical for effective treatment and prevention of recurrence.
1. Initial Clinical Assessment
a. Rapid Neurological Examination
The first step in diagnosing a stroke is a quick but focused neurological exam. Medical professionals use standard protocols to evaluate the patient’s condition within seconds to minutes of presentation.
NIH Stroke Scale (NIHSS):
A 15-item neurological exam that assesses:Consciousness
Vision
Facial palsy
Motor strength (arms and legs)
Coordination
Sensation
Language and speech
Attention
NIHSS scores range from 0 to 42:
0–4: Minor stroke
5–15: Moderate stroke
16–20: Moderate to severe
21: Severe stroke
This scoring helps determine stroke severity and guide decisions about thrombolysis and other interventions.
b. Medical History and Timeline
- Onset of symptoms: Critical for determining eligibility for time-sensitive treatments like tPA (tissue plasminogen activator).
- Prior history: Stroke, TIA, atrial fibrillation, heart disease, hypertension, diabetes, smoking, or previous neurological conditions.
- Current medications: Especially anticoagulants or antiplatelet drugs.
2. Imaging Studies
Imaging is indispensable for confirming the stroke, identifying its type (ischemic vs. hemorrhagic), and planning treatment.
a. Non-Contrast CT (Computed Tomography) of the Brain
- First-line test for most stroke patients.
- Fast and widely available.
- Primarily used to exclude hemorrhage.
- In early ischemic stroke, a CT may appear normal; changes may develop after several hours.
b. MRI (Magnetic Resonance Imaging) of the Brain
- More sensitive than CT for detecting early ischemic changes.
- Can identify small infarcts and differentiate between old and new strokes.
- Diffusion-weighted imaging (DWI): Detects ischemic changes within minutes.
- Fluid-attenuated inversion recovery (FLAIR): Useful for timing of stroke onset in uncertain cases.
c. CT Angiography (CTA) and MR Angiography (MRA)
- Visualize intracranial and extracranial vessels.
- Detect arterial occlusions, stenosis, aneurysms, or dissection.
- Critical for deciding eligibility for mechanical thrombectomy.
d. CT Perfusion or MR Perfusion Imaging
- Evaluates blood flow and helps identify penumbra (salvageable tissue).
- Helps select patients for late-window interventions (e.g., beyond 6 hours after symptom onset).
e. Carotid Doppler Ultrasound
- Assesses the carotid arteries in the neck for narrowing (stenosis) or blockage.
- Helps identify candidates for carotid endarterectomy or stenting.
3. Laboratory and Blood Tests
Essential for ruling out stroke mimics, assessing risk, and preparing for interventions.
Blood glucose: To rule out hypoglycemia, a stroke mimic.
Complete blood count (CBC): To check for anemia, infection, or polycythemia.
Electrolytes and renal function: To evaluate overall health and medication suitability.
Coagulation profile:
INR/PT, aPTT: Important if considering tPA or if patient is on anticoagulants.
Cardiac enzymes (e.g., troponin): Elevated in concurrent myocardial infarction (common in stroke patients).
Lipid profile: Assess cardiovascular risk.
ESR/CRP: May help identify vasculitis in atypical stroke presentations.
4. Cardiac Evaluation
The heart is a major source of emboli in ischemic strokes. Evaluating heart function and rhythm is key in identifying stroke etiology.
a. Electrocardiogram (ECG)
Detects atrial fibrillation, recent myocardial infarction, left ventricular hypertrophy, or other arrhythmias.
b. Echocardiography
- Transthoracic echocardiography (TTE): Evaluates heart wall motion, clots, valve problems, and overall function.
- Transesophageal echocardiography (TEE): Provides better views of the left atrium and aorta. Can detect cardiac thrombi, PFO (patent foramen ovale), and atrial septal aneurysm.
c. Holter Monitor or Continuous ECG Monitoring
- Detects paroxysmal atrial fibrillation or other intermittent arrhythmias not caught during a brief ECG.
- In cryptogenic strokes, prolonged monitoring may be required (up to 30 days).
5. Advanced Diagnostic Tools and Workup
In cases where the cause of stroke is unclear (cryptogenic), or when unusual causes are suspected, further tests may be performed.
a. Hypercoagulability Panel
Especially in young patients with no apparent risk factors.
Tests for:
Protein C and S deficiency
Antithrombin III deficiency
Factor V Leiden mutation
Antiphospholipid antibodies
b. Autoimmune and Inflammatory Screening
- Antinuclear antibody (ANA), rheumatoid factor (RF), ANCA, and others.
- Looks for vasculitis or autoimmune diseases (e.g., lupus).
c. Cerebral Angiography (Digital Subtraction Angiography)
- Invasive, gold standard for diagnosing arteriovenous malformations (AVMs), vasculitis, aneurysms, or arterial dissections.
- Mainly used when non-invasive imaging is inconclusive.
d. Lumbar Puncture
- Indicated when subarachnoid hemorrhage (SAH) is suspected but CT is negative.
- Xanthochromia (yellow discoloration of cerebrospinal fluid) confirms SAH.
6. Differential Diagnosis: Stroke Mimics
It’s important to distinguish stroke from other conditions that can produce similar symptoms:
| Condition | Key Features |
|---|---|
| Hypoglycemia | Sudden confusion, weakness; improves with glucose |
| Migraine with aura | Gradual onset, visual changes, often recurrent |
| Seizures and postictal paralysis (Todd’s paresis) | Focal weakness after a seizure |
| Brain tumor or abscess | Gradual onset, headache, possible fever |
| Multiple sclerosis | Episodic neurological symptoms, often in young adults |
| Conversion disorder | Neurological symptoms without a physiological cause |
Rapid imaging and testing help rule these out.
7. Time is Brain: The Diagnostic Timeline
The aim in acute stroke care is “door-to-needle” time of less than 60 minutes for tPA administration. A typical workflow:
- Within 10 minutes: Initial evaluation and vital signs
- Within 25 minutes: CT scan performed
- Within 45 minutes: Lab results and imaging interpreted
- Within 60 minutes: tPA administered if eligible
For thrombectomy candidates, rapid CTA/MRA and transfer to a specialized stroke center are necessary.
Treatment of Stroke
Effective treatment of stroke hinges on three essential principles:
- Speed – The faster treatment begins, the better the outcomes.
- Precision – Treatment depends on the type and cause of the stroke.
- Multidisciplinary care – Recovery involves a team including neurologists, emergency physicians, nurses, therapists, and sometimes surgeons.
Stroke treatment is primarily categorized based on stroke type:
- Ischemic Stroke – Caused by a blockage
- Hemorrhagic Stroke – Caused by bleeding
- Transient Ischemic Attack (TIA) – A temporary blockage with no lasting damage
1. Treatment of Ischemic Stroke
Ischemic strokes account for approximately 87% of all strokes and are caused by a clot blocking blood flow to the brain. Treatment goals include restoring perfusion, minimizing brain damage, and preventing recurrence.
A. Acute Treatments
a. Intravenous Thrombolysis (IV tPA)
Tissue Plasminogen Activator (tPA) is a clot-dissolving drug that must be administered within 4.5 hours of symptom onset.
Best outcomes are achieved if given within 60 minutes of hospital arrival.
Criteria for tPA administration:
Confirmed ischemic stroke via CT (no hemorrhage)
Onset of symptoms within 4.5 hours
No recent surgery or bleeding disorders
Brand names: Alteplase, Tenecteplase (in some settings)
b. Mechanical Thrombectomy
- A minimally invasive surgical procedure to physically remove a large clot from an artery in the brain using a stent retriever.
- Indicated in large-vessel occlusion (LVO) strokes in the anterior circulation.
- Can be performed up to 24 hours after symptom onset in selected patients (with CT perfusion showing salvageable tissue).
- Performed in a specialized neurointerventional suite by a neuroradiologist or neurosurgeon.
c. Bridging Therapy
Some patients receive both tPA and mechanical thrombectomy if imaging suggests both therapies are appropriate.
B. Supportive Care During Acute Phase
- Blood pressure control: Elevated BP is common but typically not lowered unless >220/120 mmHg, unless tPA is administered (then BP must be <185/110 mmHg).
- Glucose management: Maintain normoglycemia to avoid worsening outcomes.
- Oxygen and airway support: Provided if hypoxia or decreased consciousness.
- Temperature control: Fever management to avoid metabolic stress on injured brain tissue.
C. Antithrombotic Therapy (Post-Acute Phase)
a. Antiplatelet Agents
- Used to prevent new clot formation.
- First-line agents: Aspirin, Clopidogrel, or a combination for short-term use.
- Aspirin is often given within 24–48 hours of symptom onset (after excluding hemorrhage).
- Dual antiplatelet therapy (DAPT) may be used for 21–90 days in minor strokes or high-risk TIA.
b. Anticoagulation
- Used when stroke is due to cardioembolic causes (like atrial fibrillation).
- Warfarin or Direct Oral Anticoagulants (DOACs): apixaban, rivaroxaban, dabigatran.
- Usually initiated after several days, depending on infarct size and bleeding risk.
D. Statin Therapy
High-intensity statins (e.g., atorvastatin 80 mg) are initiated in most ischemic stroke patients to:
Lower LDL cholesterol
Stabilize atherosclerotic plaques
Reduce risk of future strokes
E. Surgical and Endovascular Options (Long-Term)
- Carotid Endarterectomy (CEA): Removal of plaque from carotid artery; indicated for 70–99% stenosis.
- Carotid Artery Stenting: An alternative for patients at high surgical risk.
- Patent Foramen Ovale (PFO) closure: Considered in selected younger patients with cryptogenic stroke and a confirmed PFO.
2. Treatment of Hemorrhagic Stroke
Hemorrhagic strokes account for approximately 13% of all strokes, with higher fatality and complication rates. Treatment is focused on controlling bleeding, reducing intracranial pressure, and preventing rebleeding.
A. Acute Management
a. Blood Pressure Control
- Aim to reduce systolic BP to <140 mmHg (depending on guidelines).
- IV medications: Nicardipine, Labetalol, Clevidipine.
b. Reversal of Anticoagulation
Critical if the patient is on blood thinners:
Vitamin K and Prothrombin Complex Concentrate (PCC) for warfarin reversal
Idarucizumab for dabigatran
Andexanet alfa for apixaban/rivaroxaban
c. Intracranial Pressure (ICP) Management
- Head elevation to 30 degrees
- Hyperosmolar therapy (e.g., mannitol, hypertonic saline)
- Possible sedation or intubation
B. Surgical Interventions
a. Craniotomy
Open surgery to remove a blood clot or relieve pressure from swelling.
b. External Ventricular Drain (EVD)
Drains cerebrospinal fluid (CSF) in case of hydrocephalus (especially in subarachnoid hemorrhage).
c. Aneurysm Repair
Surgical clipping or endovascular coiling to prevent rupture or re-bleeding of aneurysms.
C. Management of Subarachnoid Hemorrhage (SAH)
- Nimodipine: A calcium channel blocker given to reduce the risk of vasospasm, which can cause delayed ischemic strokes after SAH.
- ICU monitoring for at least 14 days.
- Serial imaging and transcranial Dopplers to assess vasospasm and bleeding progression.
3. Treatment of Transient Ischemic Attack (TIA)
While TIAs resolve spontaneously, they are urgent warning signs of an impending stroke. Prompt management can prevent a full-blown stroke.
A. Risk Assessment Tools
ABCD2 score helps predict short-term stroke risk based on:
- Age
- Blood pressure
- Clinical features
- Duration of symptoms
- Diabetes status
B. Management Includes:
- Immediate imaging (CT or MRI)
- Cardiac evaluation (ECG, echocardiogram)
- Carotid ultrasound
- Antiplatelet therapy
- Lifestyle modification and risk factor management
Patients with high-risk TIA may require hospitalization and urgent intervention.
4. Post-Acute Stroke Care and Secondary Prevention
Once the acute event is managed, the focus shifts to:
A. Secondary Prevention
- Blood pressure control
- Cholesterol management
- Diabetes control
- Smoking cessation
- Regular exercise and healthy diet
- Medication adherence
B. Rehabilitation
- Physical therapy: Restores mobility, strength, and coordination.
- Occupational therapy: Relearns daily tasks and adapts to disability.
- Speech-language therapy: For aphasia, dysphagia, and communication disorders.
- Neuropsychological support: Addresses cognitive deficits, depression, and emotional trauma.
Rehabilitation should start as early as possible, ideally within 24–48 hours after stabilization.
5. Emerging and Experimental Treatments
A. Neuroprotective Agents
- Investigated to limit cell death in ischemic penumbra.
- Trials ongoing; none yet FDA-approved.
B. Stem Cell Therapy
Potential for regenerating damaged brain tissue in post-stroke patients.
C. Brain-Computer Interfaces (BCIs)
Assisting recovery in severe disability by translating brain activity into movement commands.
D. Artificial Intelligence (AI)
- Used in imaging interpretation (e.g., identifying clots or hemorrhages).
- May improve diagnostic speed in emergency settings.
Stroke Recovery and Rehabilitation
Stroke recovery and rehabilitation are critical components of the stroke care continuum. While acute treatment addresses the immediate threat to life and brain tissue, recovery focuses on restoring lost function, regaining independence, and enhancing quality of life. Because strokes can cause a wide range of disabilities—physical, cognitive, emotional, and communicative—rehabilitation must be individualized, multidisciplinary, and goal-oriented.
Recovery doesn’t end at hospital discharge. In fact, for many patients, it’s just the beginning of a lifelong journey.
Goals of Stroke Rehabilitation
The primary goals of stroke rehabilitation are to:
- Restore as much function as possible (motor, sensory, speech, cognitive)
- Promote independence in activities of daily living (ADLs)
- Prevent complications such as contractures, aspiration, or depression
- Support emotional and social reintegration
- Educate patients and caregivers for long-term stroke management
Phases of Stroke Recovery
Stroke recovery generally follows a non-linear course and varies from person to person. However, it typically progresses through several phases:
1. Acute Phase (First Hours to Days)
- Begins in the hospital immediately after the stroke.
- Focuses on medical stabilization, early mobilization, and basic neurological assessment.
- Rehabilitation specialists are often consulted within 24–48 hours.
2. Subacute Phase (Days to Weeks)
- Often takes place in a rehabilitation unit or skilled nursing facility.
- More intensive rehabilitation begins during this phase.
- Recovery is usually fastest during the first 3 to 6 months post-stroke.
3. Chronic Phase (Months to Years)
- Recovery continues at home or in outpatient settings.
- Focus shifts to community reintegration, long-term management, and adaptive strategies.
- Some recovery can still occur after years, especially with consistent effort and therapy.
Key Members of the Stroke Rehabilitation Team
Rehabilitation involves a multidisciplinary team approach:
| Professional | Role |
|---|---|
| Physiatrist | Leads rehabilitation planning and coordination |
| Neurologist | Oversees neurological aspects and manages secondary prevention |
| Physical Therapist (PT) | Focuses on mobility, balance, strength, and walking |
| Occupational Therapist (OT) | Helps with self-care tasks like dressing, bathing, and using tools |
| Speech-Language Pathologist (SLP) | Addresses speech, language, cognition, and swallowing disorders |
| Neuropsychologist | Assesses cognitive and emotional function and provides therapy |
| Rehabilitation Nurse | Provides ongoing care and patient education |
| Social Worker/Case Manager | Facilitates discharge planning, community support, and resources |
| Dietitian | Helps manage nutrition, swallowing safety, and cardiovascular health |
Types of Rehabilitation Therapies
1. Physical Therapy (PT)
Aims to restore motor control, balance, and mobility.
Interventions include:
Strengthening exercises
Gait training with walkers or braces
Balance training to prevent falls
Functional electrical stimulation (FES)
Range of motion (ROM) exercises to prevent stiffness
2. Occupational Therapy (OT)
Focuses on regaining independence in Activities of Daily Living (ADLs):
Eating, bathing, grooming, dressing, and toileting
Uses adaptive devices (e.g., one-handed utensils, dressing aids)
Includes upper limb therapy for fine motor skills and coordination
3. Speech and Language Therapy (SLP)
Critical for individuals with:
Aphasia (loss of ability to understand or express language)
Dysarthria (slurred or slow speech due to muscle weakness)
Dysphagia (difficulty swallowing, which can lead to aspiration pneumonia)
Therapy may involve:
Language exercises
Communication aids (e.g., picture boards, speech-generating devices)
Swallowing exercises and modified diets
4. Cognitive and Neuropsychological Rehabilitation
Focuses on:
Memory
Attention and concentration
Problem-solving
Executive function
May involve paper-based tasks, computer exercises, and real-world training
Tailored programs help with returning to work or managing finances
5. Emotional and Psychological Support
Depression, anxiety, emotional lability, and post-stroke fatigue are common.
Treatment may involve:
Counseling or psychotherapy
Cognitive-behavioral therapy (CBT)
Medications (antidepressants, anxiolytics)
Support groups provide connection, encouragement, and shared coping strategies
Common Challenges and Complications in Stroke Recovery
- Hemiparesis/Hemiplegia: Weakness or paralysis on one side
- Spasticity: Stiff muscles that resist movement
- Pain syndromes: Shoulder pain, neuropathic pain
- Incontinence: Bladder or bowel control issues
- Visual field cuts: Partial vision loss (e.g., hemianopia)
- Neglect syndrome: Lack of awareness of one side (usually left)
- Post-stroke depression: Affects ~30–50% of stroke survivors
Management includes medications, botulinum toxin injections for spasticity, assistive technology, and family education.
Recovery Timeline and Prognosis
Recovery depends on stroke severity, location, age, pre-stroke health, and access to therapy. While most neurological recovery occurs within the first 6 months, continued improvements are possible for years.
| Time Frame | Typical Progress |
|---|---|
| 0–2 weeks | Stabilization, early mobility, initial therapy |
| 2–12 weeks | Rapid gains in strength, mobility, language |
| 3–6 months | Functional recovery in ADLs, potential return home |
| 6+ months | Ongoing therapy, adaptation, community reintegration |
Approximately:
- 10% fully recover
- 25% recover with minor impairments
- 40% have moderate to severe impairments
- 15% require long-term care
- 10% experience recurrence or complications
Home-Based and Community Rehabilitation
After discharge, therapy may continue through:
- Outpatient clinics
- Home-based rehab programs
- Tele-rehabilitation (especially important for rural or mobility-limited patients)
- Day rehabilitation programs (day hospitals or centers)
Assistive devices may include:
- Walkers, wheelchairs
- Communication boards
- Smart home technology
Home adaptations (e.g., grab bars, ramps, non-slip floors) can greatly improve safety and independence.
Innovations in Stroke Rehabilitation
- Robotics and Exoskeletons: Improve walking and limb movement through repetitive training.
- Virtual Reality (VR): Simulates real-world tasks in an immersive, motivating way.
- Brain-Computer Interfaces (BCI): Translate brain signals into movements or commands—particularly promising for severe disability.
- Transcranial Magnetic Stimulation (TMS) and tDCS: Non-invasive brain stimulation to enhance neuroplasticity.
- AI-guided therapy: Customizes rehab programs based on real-time performance.
The Role of Caregivers and Support Systems
Caregivers play an indispensable role in stroke recovery. They often provide:
- Emotional support
- Physical assistance
- Medication management
- Transportation to appointments
Caregiver burnout is common, and support groups or respite services are essential.
Reintegration and Quality of Life
Long-term goals focus on returning to work, resuming hobbies, and rebuilding relationships. For many, stroke marks a major life transition, and success is measured not only by mobility but by life satisfaction, autonomy, and social connection.
Tips for Supporting Stroke Survivors:
- Celebrate small milestones
- Encourage consistent therapy
- Promote socialization and engagement
- Respect autonomy and decision-making
Stroke Prevention
Stroke is often thought of as a sudden, unpredictable event—but in reality, the majority of strokes are preventable. Research shows that up to 80% of strokes can be prevented by addressing modifiable risk factors and adopting healthy lifestyle habits. Stroke prevention is not a one-size-fits-all strategy—it requires personalized, ongoing efforts and support at both the individual and population levels.
Stroke prevention is divided into two categories:
- Primary prevention: Preventing the first stroke in individuals at risk.
- Secondary prevention: Preventing recurrence in those who have already had a stroke or TIA.
Primary Stroke Prevention
A. Lifestyle Modifications
1. Control Blood Pressure (Hypertension)
High blood pressure is the leading risk factor for both ischemic and hemorrhagic strokes.
Goal: Keep blood pressure below 130/80 mmHg for most individuals.
Strategies:
Reduce salt intake (<2,300 mg/day or ideally <1,500 mg/day)
Increase potassium-rich foods (bananas, spinach)
Exercise regularly
Take prescribed antihypertensive medications consistently
Monitor at home with a validated blood pressure monitor
2. Quit Smoking
Smoking doubles the risk of stroke and accelerates atherosclerosis.
Quitting reduces risk significantly within 2–5 years.
Supportive resources:
Behavioral therapy
Nicotine replacement products (patches, gum)
Prescription medications (e.g., bupropion, varenicline)
3. Eat a Heart-Healthy Diet
Focus on diets that reduce cholesterol, blood pressure, and inflammation:
DASH (Dietary Approaches to Stop Hypertension)
Mediterranean Diet
Dietary tips:
Increase: Fruits, vegetables, whole grains, legumes, lean proteins (fish, poultry), nuts
Decrease: Red meat, processed foods, sugary beverages, trans fats, excessive alcohol
4. Maintain a Healthy Weight
- Obesity increases the risk of stroke by promoting diabetes, hypertension, and high cholesterol.
- Aim for a BMI between 18.5–24.9 and waist circumference <35 inches (women) or <40 inches (men).
- Sustainable strategies include portion control, physical activity, and medical or surgical options if needed.
5. Exercise Regularly
Regular physical activity improves cardiovascular health, reduces inflammation, and regulates glucose and lipid metabolism.
Recommendation:
At least 150 minutes/week of moderate-intensity aerobic activity
Include strength training 2 days/week
6. Limit Alcohol Intake
Heavy drinking raises blood pressure and increases stroke risk.
Safe limits:
Men: No more than 2 standard drinks/day
Women: No more than 1 standard drink/day
Binge drinking should be avoided completely.
7. Manage Stress and Mental Health
Chronic stress contributes to high blood pressure and unhealthy habits.
Techniques:
Mindfulness meditation
Cognitive-behavioral therapy
Breathing exercises and yoga
Adequate sleep and social connection
B. Medical Management of Risk Factors
1. Control Diabetes
High blood sugar damages blood vessels and accelerates atherosclerosis.
Goals:
HbA1c <7% for most adults
Blood pressure and cholesterol management
Healthy diet and medications (e.g., metformin, insulin, SGLT2 inhibitors)
2. Lower Cholesterol
High LDL cholesterol contributes to plaque buildup in arteries.
Guidelines recommend:
High-intensity statin therapy for high-risk individuals
Lifestyle changes as the first-line approach
3. Identify and Treat Atrial Fibrillation (AFib)
AFib is a major cause of embolic strokes.
Screening: ECG or wearable heart monitor in patients >65 years or those with symptoms (palpitations, dizziness).
Management:
Anticoagulants (e.g., warfarin, apixaban, rivaroxaban)
Rate and rhythm control (beta-blockers, ablation)
4. Manage Sleep Apnea
Obstructive sleep apnea is linked to stroke risk via intermittent hypoxia and hypertension.
Diagnosis: Overnight sleep study (polysomnography)
Treatment: CPAP machine, weight loss, or oral appliances
5. Avoid Illegal Drugs
- Cocaine, methamphetamines, and other stimulants can cause both ischemic and hemorrhagic strokes.
- Education, counseling, and addiction support are crucial.
Secondary Stroke Prevention
For individuals who have experienced a stroke or TIA, secondary prevention aims to prevent recurrence, which is often more severe or fatal.
A. Antithrombotic Therapy
1. Antiplatelet Agents
Used in non-cardioembolic ischemic strokes.
Options include:
Aspirin
Clopidogrel
Aspirin + dipyridamole
Dual antiplatelet therapy (DAPT) may be used for 21–90 days after minor stroke or high-risk TIA.
2. Anticoagulation
For cardioembolic strokes due to AFib or other heart conditions.
Medications:
Warfarin
DOACs: apixaban, rivaroxaban, dabigatran
INR monitoring is essential for patients on warfarin.
B. Carotid Artery Management
Carotid stenosis is a significant risk factor for stroke recurrence.
Interventions:
Carotid endarterectomy (surgical removal of plaque)
Carotid artery stenting (minimally invasive option)
Typically recommended for patients with >70% stenosis and recent symptoms.
C. Cardiac Source of Embolism
- Patent foramen ovale (PFO) closure may be considered in younger patients with cryptogenic stroke.
- Ongoing cardiac monitoring may detect undiagnosed AFib in cryptogenic strokes.
D. Lifestyle and Risk Factor Management
Same as primary prevention but more aggressively enforced:
Lower BP goals (<130/80 mmHg)
Strict glucose and lipid control
Tobacco and alcohol cessation
Routine physical and cognitive rehabilitation
E. Rehabilitation and Monitoring
Continued rehabilitation helps reduce the risk of complications and enhances long-term recovery.
Regular follow-ups to monitor:
Medication adherence
Mental health
Vascular imaging (carotid ultrasound, echocardiography)
Lab values (HbA1c, lipid panels, renal function)
Community and Public Health Strategies
Effective stroke prevention also requires a broader public health approach to address social determinants and systemic barriers.
A. Public Awareness Campaigns
- Educate about stroke signs and prevention (e.g., FAST campaigns)
- Encourage routine screening for BP, cholesterol, and diabetes
B. Community Health Programs
- Free or low-cost BP screening at pharmacies and clinics
- Culturally tailored health education for at-risk populations
- Support for smoking cessation and exercise programs
C. Policy-Level Interventions
- Regulation of salt, trans fats, and sugar in processed foods
- Urban design to promote physical activity (parks, walking paths)
- Subsidies for healthy foods in underserved areas
- Mandatory AFib screening in adults >65
Screening Recommendations
| Risk Factor | Screening Tool | Frequency |
|---|---|---|
| Hypertension | Blood pressure measurement | At every doctor’s visit or annually |
| Diabetes | Fasting glucose, HbA1c | Every 3 years (more if high risk) |
| Atrial Fibrillation | Pulse check, ECG, Holter | Annually for >65 or symptomatic |
| Cholesterol | Lipid panel | Every 4–6 years (more if abnormal) |
| Sleep Apnea | Sleep study | If symptoms or high risk |
| Carotid Artery Disease | Carotid ultrasound | If symptomatic or >70% stenosis |