
Oral cancer remains a significant global health burden, particularly in regions with high prevalence of tobacco use, alcohol consumption, betel nut chewing, and poor oral health awareness. A crucial aspect of reducing morbidity and mortality associated with oral squamous cell carcinoma (OSCC) lies in the early identification and management of premalignant (potentially malignant) oral lesions. These lesions represent a spectrum of disorders affecting the oral mucosa that carry an increased risk of malignant transformation, although not all inevitably progress to cancer.
The term premalignant lesion does not imply certainty of cancer development. In fact, only a small proportion of oral cancers arise from clinically identifiable premalignant lesions. Nevertheless, their recognition is essential because malignant transformation, when it occurs, can be life-threatening. Appropriate diagnosis, timely intervention, modification of risk factors, and long-term surveillance are therefore central to patient care.
Table of Contents
ToggleConcept of Premalignant Oral Lesions
Premalignant lesions are defined as morphologically altered tissues in which cancer is more likely to occur than in their apparently normal counterparts. These lesions arise due to chronic irritation, chemical exposure, infections, immunological factors, or genetic abnormalities.
It is important to distinguish between:
- Premalignant lesions (localized tissue changes, e.g. leukoplakia)
- Premalignant conditions (generalized disorders associated with increased cancer risk, e.g. submucous fibrosis)
Despite heightened attention to these entities, most individuals diagnosed with premalignant lesions do not progress to oral cancer. However, the challenge lies in identifying which lesions are more likely to undergo malignant change.
Leucoplakia
Definition
Leucoplakia is defined by the World Health Organization (WHO) as:
“A white patch or plaque that cannot be characterized clinically or pathologically as any other disease.”
This definition emphasizes exclusion, meaning leukoplakia is diagnosed only after ruling out other causes of white oral lesions such as candidiasis, lichen planus, frictional keratosis, or chemical burns.
Epidemiology
Leucoplakia affects approximately 3% of the white population, with higher prevalence in populations exposed to tobacco, betel nut, or alcohol. It commonly affects middle-aged and older adults and shows a male predominance in many regions.
Clinical Features
Leucoplakia typically presents as:
- A white, non-scrapable patch or plaque
- Well-demarcated or irregular margins
- Smooth, fissured, nodular, or verrucous surface
Common intraoral sites include:
- Buccal mucosa
- Floor of the mouth
- Ventral surface of the tongue
- Gingiva and alveolar mucosa
Lesions involving the floor of the mouth and ventral tongue are particularly concerning due to their higher malignant potential.
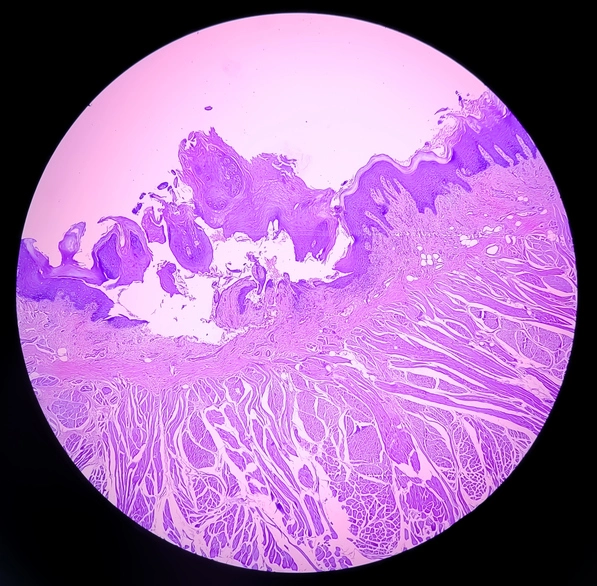
Histopathology
Histopathological findings in leucoplakia vary widely, ranging from benign hyperkeratosis to carcinoma in situ. Typical microscopic features include:
- Thickened keratin layer (hyperkeratosis)
- Thickening of the prickle cell layer (acanthosis)
- Inflammatory infiltrate in the connective tissue (often plasma cells)
The most critical histological determinant of risk is the presence and degree of epithelial dysplasia.
Epithelial Dysplasia: Key Features
Epithelial dysplasia reflects disordered growth and maturation of epithelial cells. Important microscopic features include:
- Nuclear hyperchromatism
- Increased nuclear-to-cytoplasmic ratio
- Cellular and nuclear pleomorphism
- Increased and/or atypical mitotic figures
- Individual cell keratinization
- Loss of normal cell polarity
- Disturbance of cell adhesion and arrangement
Dysplasia is graded as mild, moderate, or severe, although there is significant inter- and intra-observer variability among pathologists. Furthermore, a biopsy sample may not be representative of the entire lesion, posing a diagnostic challenge.
Malignant Transformation Risk
Meta-analyses indicate:
- Overall malignant transformation rate: ~12%
- Mild/moderate dysplasia: ~10%
- Severe dysplasia: ~24%
Certain sites, particularly the floor of the mouth, show transformation rates exceeding 25%. Some variants, such as candidal leukoplakia, have reported malignant transformation rates as high as 30–40%.
Interestingly, malignant transformation appears to be more common in non-smokers, possibly reflecting idiopathic leukoplakia with underlying genetic instability.
Diagnosis and Management
Specialist referral is essential. Management typically includes:
- Incisional or excisional biopsy
- Use of toluidine blue staining to guide biopsy site
- Elimination of etiological factors (tobacco, alcohol, betel nut)
Treatment options depend on histological findings and may include:
- Surgical excision
- Laser ablation
- Cryotherapy
- Medical therapy (retinoids, beta-carotene, lycopene)
Erythroleucoplakia (Speckled Leucoplakia)
Erythroleucoplakia refers to a lesion that exhibits both white (leucoplakic) and red (erythroplakic) components. The presence of red areas signifies epithelial thinning and increased vascular visibility, which correlates with a significantly higher risk of malignant transformation compared to homogeneous leukoplakia.
These lesions demand urgent biopsy and aggressive management.
Erythroplakia
Definition
Erythroplakia is defined as:
“A bright red, velvety plaque that cannot be characterized clinically or pathologically as any other recognizable condition.”
Clinical Importance
Erythroplakia is far less common than leukoplakia but carries an extremely high malignant potential. Studies indicate that at least 85% of erythroplakic lesions show:
- Severe epithelial dysplasia
- Carcinoma in situ
- Invasive carcinoma
Common Sites
- Floor of the mouth
- Ventral tongue
- Soft palate
Because of its high-risk nature, erythroplakia should always be considered malignant until proven otherwise.
Management
Immediate biopsy is mandatory. Treatment usually involves:
- Wide surgical excision
- Close postoperative surveillance
- Elimination of risk factors
Erosive Lichen Planus
Lichen planus is a chronic inflammatory condition affecting skin and mucous membranes. The erosive form is comparatively rare but clinically significant.
Malignant Potential
- Estimated risk of malignant transformation: <1%
- Non-erosive forms (reticular, papular) have no proven premalignant potential
Clinical Features
Erosive lichen planus presents with:
- Painful erythematous and ulcerated areas
- Peripheral white striae (Wickham’s striae)
- Burning sensation, especially with spicy foods
Management
Management focuses on:
- Symptom control (topical/systemic corticosteroids)
- Monitoring for dysplastic changes
- Regular follow-up and biopsy of suspicious areas
Oral Submucous Fibrosis
Epidemiology and Etiology
Oral submucous fibrosis (OSF) is predominantly seen in individuals of South Asian origin. It is strongly associated with areca nut (betel nut) chewing, with or without tobacco.
Pathogenesis
The disease is characterized by:
- Chronic inflammation
- Fibroblast hyperplasia
- Excess collagen deposition
Areca nut contains copper, which increases lysyl oxidase activity, leading to enhanced collagen cross-linking, fibrosis, and potential DNA damage.
Clinical Features
- Pale, stiff oral mucosa
- Fibrous bands in buccal mucosa and lips
- Progressive reduction in mouth opening (trismus)
- Burning sensation
Histology
- Epithelial atrophy
- Cellular atypia
- Dense collagen deposition in submucosa
Malignant Transformation
- Transformation rate: ~10%
- Time frame: 10–15 years
Management
Treatment includes:
- Cessation of betel nut and tobacco use
- Intralesional corticosteroids
- Physiotherapy and mouth-opening exercises
- Surgical release of fibrous bands with flap reconstruction in advanced cases
Dyskeratosis Congenita
Dyskeratosis congenita is a rare autosomal dominant genetic disorder characterized by:
- Skin pigmentation abnormalities
- Nail dystrophy
- Oral leukoplakia appearing in childhood
The oral white plaques have premalignant potential, necessitating lifelong surveillance.
Patterson–Brown–Kelly (Plummer–Vinson) Syndrome
This syndrome is characterized by:
- Iron deficiency anemia
- Dysphagia
- Esophageal webs
It is associated with an increased risk of upper aerodigestive tract cancers, including oral and pharyngeal carcinoma.
Management Principles of Premalignant Oral Lesions
Effective management requires an individualized, evidence-based approach.
Assessment
- Accurate documentation of lesion site and size
- Photographic records
- Histopathological evaluation
- Consideration of patient age, health, and habits
Risk Factor Modification
- Complete cessation of smoking
- Elimination of alcohol abuse
- Discontinuation of betel nut chewing
- Nutritional optimization
Surveillance
- Regular clinical examinations
- Repeat biopsy if clinical changes occur
- Three-monthly follow-up intervals are commonly recommended
Therapeutic Options
- Surgical excision
- Laser therapy
- Cryotherapy
- Medical therapy (retinoids, antioxidants)
The choice depends on lesion type, dysplasia severity, and patient factors.
Conclusion
Premalignant lesions of the oral cavity represent a critical window of opportunity for cancer prevention. While not all lesions progress to malignancy, their unpredictable behavior necessitates vigilance, early diagnosis, and long-term follow-up. A thorough understanding of their clinical presentation, histopathology, and risk factors enables clinicians to intervene appropriately and reduce the burden of oral cancer.
Early recognition, patient education, habit cessation, and multidisciplinary management remain the cornerstones of successful outcomes.